Slides and Transcript
Slide 1 of 13
Hello! This is Dr. David Osser from Needham, Massachusetts, United States. I’m an associate professor of Psychiatry at Harvard Medical School and I work full time at the US Department of Veterans Affairs Hospital in Brockton, Massachusetts. I would like to welcome you to this updated lecture on a psychopharmacology algorithm for the treatment of PTSD.
Slide 2 of 13
I should first mention that PTSD is associated with dysregulation of neurotransmitter, neuroendocrine, neuroanatomical systems in the brain. And therefore, pharmacotherapy has a potential role in its treatment but it’s not necessarily first line or even necessarily needed. Psychotherapeutic modalities are very important in the treatment of PTSD and may be primary.
References:
- Bajor, L. A., Balsara, C., & Osser, D. N. (2025). Posttraumatic Stress Disorder Psychopharmacology Algorithm Update-2024-2025. Psychiatry and Clinical Psychopharmacology, 35(Suppl 1), S135–S140. https://doi.org/10.5152/pcp.2025.241041
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 13
So to proceed to introduce the algorithm, I should start by pointing out that only two medications are approved by the Food and Drug Administration for PTSD and those are paroxetine and sertraline, two SSRIs. As the only two approved medications, you will find that most other algorithms and guidelines out there recommend SSRIs first line. But our focus in this algorithm on the quality of the evidence regarding SSRIs versus other medications being used and studied in PTSD led us to actually propose a treatment sequence that starts with treating sleep disturbance first, usually with prazosin. So to that extent, our algorithm is significantly different from some of the other guidelines out there and you’ll hear the full justification for that in the course of this series of talks as I present the whole algorithm.
References:
- Bajor, L. A., Balsara, C., & Osser, D. N. (2025). Posttraumatic Stress Disorder Psychopharmacology Algorithm Update-2024-2025. Psychiatry and Clinical Psychopharmacology, 35(Suppl 1), S135–S140. https://doi.org/10.5152/pcp.2025.241041
Slide 4 of 13
The first step is to confirm that the patient meets criteria for posttraumatic stress disorder in the DSM-5-TR because virtually all the evidence that we’re looking at of psychopharm studies involves studies that recruited patients that met those criteria.
References:
- Bajor, L. A., Balsara, C., & Osser, D. N. (2025). Posttraumatic Stress Disorder Psychopharmacology Algorithm Update-2024-2025. Psychiatry and Clinical Psychopharmacology, 35(Suppl 1), S135–S140. https://doi.org/10.5152/pcp.2025.241041
- Mann, S. K., Marwaha, R., & Torrico, T. J. (2024, February 25). Posttraumatic stress disorder. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK559129/
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 13
As part of the diagnostic process assess for comorbidities because there frequently are several other disorders going on at the same time as your PTSD and the presence of those may make some alteration in your basic approach. So step 1A of the algorithm is to see if they have substance use disorders, bipolar disorder, a psychosis, major depression, have dissociative symptoms or it’s a woman who is pregnant or could become pregnant.
References:
- Bajor, L. A., Balsara, C., & Osser, D. N. (2025). Posttraumatic Stress Disorder Psychopharmacology Algorithm Update-2024-2025. Psychiatry and Clinical Psychopharmacology, 35(Suppl 1), S135–S140. https://doi.org/10.5152/pcp.2025.241041
Slide 6 of 13
But having reviewed that, the basic algorithm begins with making a determination if sleep is one of the problems they’re having. And from 70% to 90% of people with PTSD do have sleep problems. Some consider this the hallmark of PTSD, the most likely area where you will find pathology that the patient will be complaining of. It’s in the population I see at our Veterans Hospital. It seems to me pretty much universal that everyone with PTSD has some level of insomnia.
References:
- Bajor, L. A., Balsara, C., & Osser, D. N. (2025). Posttraumatic Stress Disorder Psychopharmacology Algorithm Update-2024-2025. Psychiatry and Clinical Psychopharmacology, 35(Suppl 1), S135–S140. https://doi.org/10.5152/pcp.2025.241041
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 13
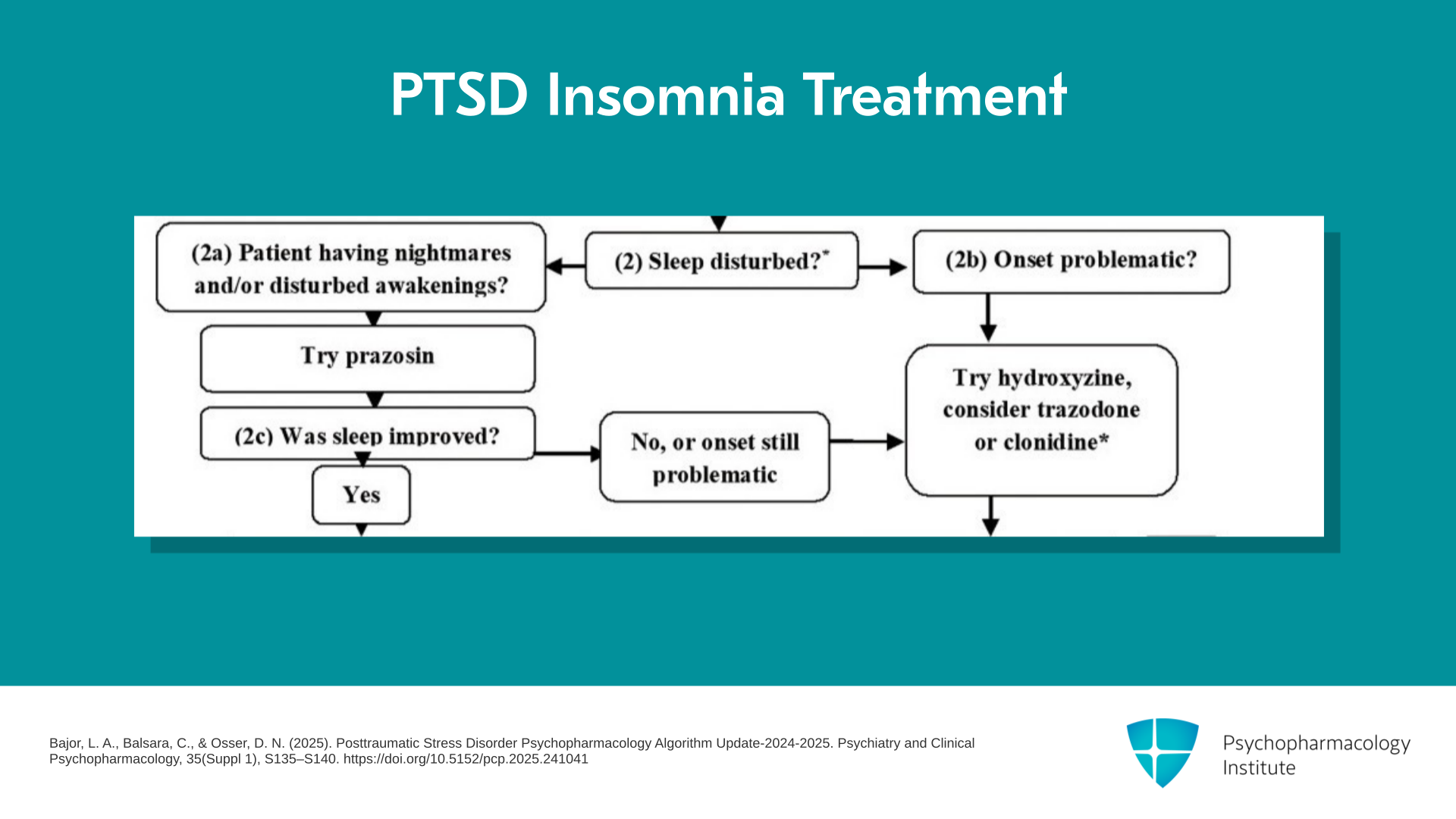
So there are two kinds of insomnia that would be of concern. One is problems falling asleep, the onset of sleep which is to the right there. And if that’s the only problem with their sleep, then we would try hydroxyzine as our first-line anti-insomnia agent for this population. We would consider trazodone or clonidine. Trazodone is very frequently used but has actually no placebo-controlled trials in PTSD so we rank it a little lower. Hydroxyzine has one trial and clonidine has experience backing it, but again no placebo-controlled trials in this population. Now, on the other side of the algorithm you see, what if the problem with sleep is problem staying asleep, waking up due to nightmares or disturbed awakenings as a result of hyperarousal? Then our first recommendation for this patient is prazosin. That’s our first medication for this patient with PTSD. But the other option on the question, was sleep improved, was either it wasn’t improved or the ability to stay asleep was improved but they still have trouble falling asleep, then the arrow takes you to the same place where if they had trouble falling asleep as their main problem which is to try hydroxyzine, trazodone or clonidine.
References:
- Bajor, L. A., Balsara, C., & Osser, D. N. (2025). Posttraumatic Stress Disorder Psychopharmacology Algorithm Update-2024-2025. Psychiatry and Clinical Psychopharmacology, 35(Suppl 1), S135–S140. https://doi.org/10.5152/pcp.2025.241041
Slide 8 of 13
And if the sleep was improved, you’re then ready to go down to the next step which is asking if this has taken care of their major PTSD symptoms as well while the sleep was improved. If there are significant remaining PTSD symptoms, you’ll go on to a trial of an SSRI as our first-line next medication. So have you given an adequate trial of an SSRI is our question. We have some parameters for that. If the answer is yes, then the question is, what was the response? And there are several possibilities but the other possibility is you haven’t given an adequate trial or they’ve got bipolar disorder. If they don’t have bipolar and they have not had a trial of an SSRI, then we recommend one.
References:
- Bajor, L. A., Balsara, C., & Osser, D. N. (2025). Posttraumatic Stress Disorder Psychopharmacology Algorithm Update-2024-2025. Psychiatry and Clinical Psychopharmacology, 35(Suppl 1), S135–S140. https://doi.org/10.5152/pcp.2025.241041
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 9 of 13
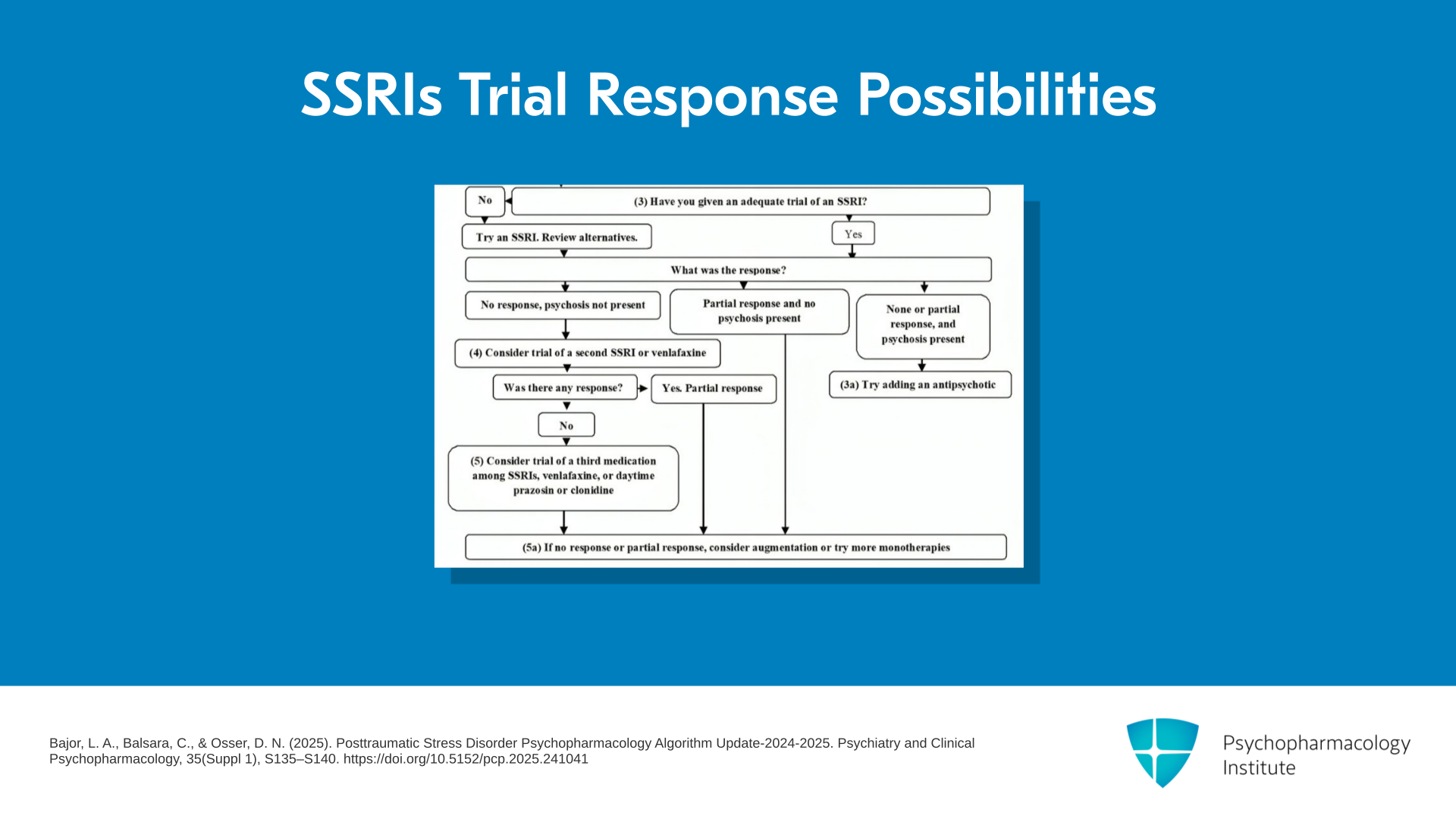
So what happened with that trial? Three possibilities. They could’ve had no response and this is a patient without comorbid psychosis. Or they could’ve had no response and there is psychosis present.
References:
- Bajor, L. A., Balsara, C., & Osser, D. N. (2025). Posttraumatic Stress Disorder Psychopharmacology Algorithm Update-2024-2025. Psychiatry and Clinical Psychopharmacology, 35(Suppl 1), S135–S140. https://doi.org/10.5152/pcp.2025.241041
Slide 10 of 13
Now, you can get psychosis with PTSD. You do have to determine if it’s not due to another disorder where the psychotic symptoms are primary like schizophrenia. Then the algorithm would not apply. You should be using your schizophrenia algorithm. But there are psychotic symptoms associated with PTSD. And in that case, we recommend adding an antipsychotic, probably aripiprazole is the recommendation. Notice that we did recommend an SSRI even if they had psychosis to be tried first because sometimes the psychosis will improve when you treat the whole syndrome of PTSD with psychosis. But if it does not, if the psychosis is still present, then we would add an antipsychotic.
References:
- Bajor, L. A., Balsara, C., & Osser, D. N. (2025). Posttraumatic Stress Disorder Psychopharmacology Algorithm Update-2024-2025. Psychiatry and Clinical Psychopharmacology, 35(Suppl 1), S135–S140. https://doi.org/10.5152/pcp.2025.241041
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 11 of 13
But another possible answer to the question, was there a response to the antidepressant, could be there was no response and there was no psychosis present. So what will we give for our second trial of a medication for the remaining symptoms of PTSD after you tried prazosin for, or otherwise treated the sleep problem? And if the answer is you have not tried a second med, then we would recommend trying a second different SSRI or you could try an SNRI. If the answer is there was response, then you would maintain the patient on that.
References:
- Bajor, L. A., Balsara, C., & Osser, D. N. (2025). Posttraumatic Stress Disorder Psychopharmacology Algorithm Update-2024-2025. Psychiatry and Clinical Psychopharmacology, 35(Suppl 1), S135–S140. https://doi.org/10.5152/pcp.2025.241041
Slide 12 of 13
But if not, you could go to your third trial which is yet another choice from among SSRIs, SNRIs. Or if you haven’t tried it yet, you could try prazosin in the daytime. You might have wound up doing that right at the beginning when you were trying to treat sleep. You may have given some during the day. Some people might choose to do that. There is a moderate amount of evidence that it can work for regular daytime symptoms. So we’re having it here as an option formally for the third trial if you didn’t try it earlier. And the last option about response to the SSRIs, what if it was a partial response, then we have a variety of augmentation options and other monotherapies which I will be describing in more detail when I go through the steps in more detail in the next several talks.
References:
- Bajor, L. A., Balsara, C., & Osser, D. N. (2025). Posttraumatic Stress Disorder Psychopharmacology Algorithm Update-2024-2025. Psychiatry and Clinical Psychopharmacology, 35(Suppl 1), S135–S140. https://doi.org/10.5152/pcp.2025.241041
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 13 of 13
So this concludes the introduction. I’d want to repeat the key points that I’ve just made. The first is that this algorithm is meant to help clinicians decide what to prescribe for second and third if you and the patient agree to try medication. But it should not be taken to imply that we think you should always use medication or that if it is used it would be first line over psychotherapy. The most important though and for some clinicians perhaps new aspect of this algorithm compared to other guidelines that are out there is the emphasis on the use of prazosin early because it has the strongest evidence of efficacy and safety for PTSD particularly for sleep.