
Slides and Transcript
Slide 1 of 14
This is a continuation of the algorithm for psychopharmacology of PTSD, and in this section we’re going to discuss what to do if a patient has been treated with an SSRI and they have psychotic symptoms connected with their PTSD.
Slide 2 of 14
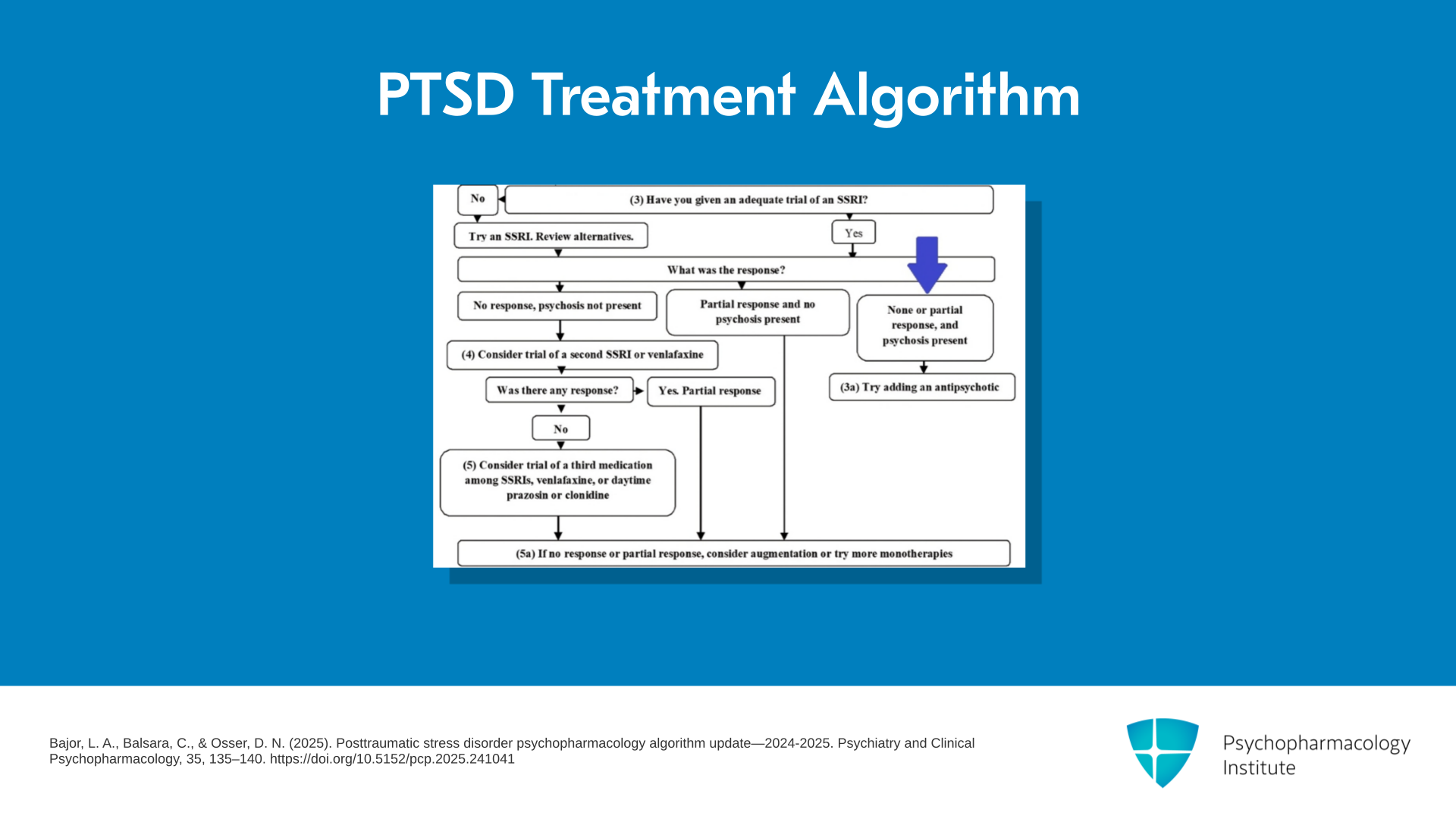
I show you the flowchart again, and I have got a blue arrow showing you where we are in the algorithm. They had been given an adequate trial of an SSRI and their response was either no response, or they had a partial response to the SSRI and they have psychosis. And we have the psychosis here because PTSD-related psychotic symptoms actually might respond to the SSRI but if there was no response of anything, we are going to tell you what we think is best.
References:
- Bajor, L. A., Balsara, C., & Osser, D. N. (2025). Posttraumatic stress disorder psychopharmacology algorithm update—2024-2025. Psychiatry and Clinical Psychopharmacology, 35, 135–140. https://doi.org/10.5152/pcp.2025.241041
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 14
But first, I want to give some examples of PTSD-related psychotic symptoms that have been described in the papers on this. The Yale group has been particularly interested, under Mark Hamner, in this subgroup of PTSD people who have psychosis. So examples would include auditory hallucinations, hearing soldiers screaming. For example, you might have been on the duty to have to pick up dead bodies of soldiers in Afghanistan or their body parts and put them in bags and take them back to the base. And while you were there doing that, some other soldiers might have been alive and screaming in pain and others were tending to them. So this is the kind of traumatic experience you can have in war role.
References:
- Hamner, M. B., Frueh, B. C., Ulmer, H. G., Huber, M. G., Twomey, T. J., Tyson, C., & Arana, G. W. (2000). Psychotic features in chronic posttraumatic stress disorder and schizophrenia: Comparative severity. The Journal of Nervous and Mental Disease, 188(4), 217–221. https://doi.org/10.1097/00005053-200004000-00004
Slide 4 of 14
Another example is you’ve been attacked and assaulted as your trauma, and you may have visual hallucinations. They’re like flashbacks to this attacker being about to attack you again. Also, you might have non-bizarre delusions that relate specifically to your trauma somehow of involvement with a dangerous situation that is not bizarre. Usually, the bizarre delusions are connected with primary psychotic disorders. You can get paranoid delusions but usually they’re not associated with a flat affect or disorganized thinking that would be part of schizophrenia.
References:
- Hamner, M. B., Frueh, B. C., Ulmer, H. G., Huber, M. G., Twomey, T. J., Tyson, C., & Arana, G. W. (2000). Psychotic features in chronic posttraumatic stress disorder and schizophrenia: Comparative severity. The Journal of Nervous and Mental Disease, 188(4), 217–221. https://doi.org/10.1097/00005053-200004000-00004
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 14
So what do we have for studies of this condition? Well, actually, the best evidence is with risperidone. That has an open-label report by Dr. Hamner, and another one by Rothbaum and colleagues.
References:
- Hamner, M. B., Faldowski, R. A., Ulmer, H. G., Frueh, B. C., Huber, M. G., & Arana, G. W. (2003). Adjunctive risperidone treatment in post-traumatic stress disorder: A preliminary controlled trial of effects on comorbid psychotic symptoms. International Clinical Psychopharmacology, 18(1), 1–8. https://doi.org/10.1097/00004850-200301000-00001
- Rothbaum, B. O., Killeen, T. K., Davidson, J. R., Brady, K. T., Connor, K. M., & Heekin, M. H. (2008). Placebo-controlled trial of risperidone augmentation for selective serotonin reuptake inhibitor-resistant civilian posttraumatic stress disorder. The Journal of Clinical Psychiatry, 69(4), 520-525. https://doi.org/10.4088/jcp.v69n0402

Slide 6 of 14
Quetiapine has had open-label data. There was this study by Villarreal in 2016 where they found significant improvement in global PTSD symptoms especially re-experiencing and hyperarousal clusters, and depression and anxiety, and positive effect on psychosis but not any negative symptoms. So that is a positive study but they were a mixture of people, some of whom had positive psychotic symptoms and some did not. So it isn’t parsed out whether it was only the psychotic people that got these improvements. So in other words, quetiapine has some reasonable evidence in this study for being a good choice. Villarreal also had monotherapy data and the way they dosed it was to start with 25 mg but they did go as high as 800.
References:
- Villarreal, G., Hamner, M. B., Cañive, J. M., Robert, S., Calais, L. A., Durklaski, V., Zhai, Y., & Qualls, C. (2016). Efficacy of quetiapine monotherapy in posttraumatic stress disorder: A randomized, placebo-controlled trial. The American Journal of Psychiatry, 173(12), 1205-1212. https://doi.org/10.1176/appi.ajp.2016.15070967
- Villarreal, G., Hamner, M. B., Qualls, C., & Cañive, J. M. (2018). Characterizing the effects of quetiapine in military post-traumatic stress disorder. Psychopharmacology Bulletin, 48(2), 8-17. https://doi.org/10.64719/pb.4561
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 14
Also, quetiapine has unique effects on dopamine, serotonin, norepinephrine receptors, neuropeptide Y and CRH that could explain benefits on PTSD. Alpha-1 antagonism may help with sleep and nightmare difficulties. So quetiapine is a treatment for PTSD without a doubt, and even possibly for psychotic symptoms.
References:
- Villarreal, G., Hamner, M. B., Cañive, J. M., Robert, S., Calais, L. A., Durklaski, V., Zhai, Y., & Qualls, C. (2016). Efficacy of quetiapine monotherapy in posttraumatic stress disorder: A randomized, placebo-controlled trial. The American Journal of Psychiatry, 173(12), 1205-1212. https://doi.org/10.1176/appi.ajp.2016.15070967
- Villarreal, G., Hamner, M. B., Qualls, C., & Cañive, J. M. (2018). Characterizing the effects of quetiapine in military post-traumatic stress disorder. Psychopharmacology Bulletin, 48(2), 8-17. https://doi.org/10.64719/pb.4561
Slide 8 of 14
What about aripiprazole? Well, the evidence on risperidone and quetiapine are stronger but in general, it has fewer side effects than those two drugs. So if you’re going to use an antipsychotic, what evidence do we have on aripiprazole for psychosis? Well, we had a retrospective chart review where it helped on PTSD clusters and depression severity when added as an adjunct. The other medications were held constant, it was started at 2 to 5 mg, titrated up to an average of 12.4 at the end and there were some improvements in some rating scales.
References:
- Richardson, J. D., Fikretoglu, D., Liu, A., & McIntosh, D. (2011). Aripiprazole augmentation in the treatment of military-related PTSD with major depression: a retrospective chart review. BMC Psychiatry, 11, 86. https://doi.org/10.1186/1471-244X-11-86
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 9 of 14
And there actually is a randomized controlled trial of aripiprazole for PTSD in 16 patients, hardly any. What did it show? Non-significant improvement in PTSD symptoms, depression and psychosis, with adjunctive aripiprazole for eight weeks in this placebo-controlled trial.
References:
- Naylor, J. C., Kilts, J. D., Bradford, D. W., Strauss, J. L., Capehart, B. P., Szabo, S. T., Smith, K. D., Dunn, C. E., Conner, K. M., Davidson, J. R., Wagner, H. R., Hamer, R. M., & Marx, C. E. (2015). A pilot randomized placebo-controlled trial of adjunctive aripiprazole for chronic PTSD in US military Veterans resistant to antidepressant treatment. International Clinical Psychopharmacology, 30(3), 167–174. https://doi.org/10.1097/YIC.0000000000000061
Slide 10 of 14
So when you add all those studies up, you get a possible for aripiprazole but it does have less side effects. So what do we conclude? So in these studies, aripiprazole monotherapy is effective in PTSD and comorbid depression in some veterans.
References:
- Richardson, J. D., Fikretoglu, D., Liu, A., & McIntosh, D. (2011). Aripiprazole augmentation in the treatment of military-related PTSD with major depression: a retrospective chart review. BMC Psychiatry, 11, 86. https://doi.org/10.1186/1471-244X-11-86
- Naylor, J. C., Kilts, J. D., Bradford, D. W., Strauss, J. L., Capehart, B. P., Szabo, S. T., Smith, K. D., Dunn, C. E., Conner, K. M., Davidson, J. R., Wagner, H. R., Hamer, R. M., & Marx, C. E. (2015). A pilot randomized placebo-controlled trial of adjunctive aripiprazole for chronic PTSD in US military Veterans resistant to antidepressant treatment. International Clinical Psychopharmacology, 30(3), 167–174. https://doi.org/10.1097/YIC.0000000000000061
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 11 of 14
Naylor did a monotherapy trial with it, started with 5 mg, had a mean dose of 10 at final at week 8. It was well tolerated, reduced intensity and frequency of side effects over time, akathisia being the biggest one. Non-significant improvement in PTSD though.
References:
- Naylor, J. C., Kilts, J. D., Bradford, D. W., Strauss, J. L., Capehart, B. P., Szabo, S. T., Smith, K. D., Dunn, C. E., Conner, K. M., Davidson, J. R., Wagner, H. R., Hamer, R. M., & Marx, C. E. (2015). A pilot randomized placebo-controlled trial of adjunctive aripiprazole for chronic PTSD in US military Veterans resistant to antidepressant treatment. International Clinical Psychopharmacology, 30(3), 167–174. https://doi.org/10.1097/YIC.0000000000000061
Slide 12 of 14
There was also a study by Youssef, again monotherapy, flexible dosing, 5 to 30. Side effects included weight gain, concentration difficulties, akathisia, nausea and numbing and tingling. Significant improvement though on total CAPS scores which is a PTSD scale especially cluster B, and also PANSS improved on all three scales. So that was basically a positive study in PTSD. PANSS which measures psychotic symptoms did improve on all three subscales.
References:
- Youssef, N. A., Marx, C. E., Bradford, D. W., Zinn, S., Hertzberg, M. A., Kilts, J. D., Naylor, J. C., Butterfield, M. I., & Strauss, J. L. (2012). An open-label pilot study of aripiprazole for male and female veterans with chronic post-traumatic stress disorder who respond suboptimally to antidepressants. International Clinical Psychopharmacology, 27(4), 191–196. https://doi.org/10.1097/YIC.0b013e328352ef4e
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 13 of 14
So in conclusion, the key points of this section: Some patients with PTSD have psychotic symptoms. They are related to the traumatic events by definition. Rule out a primary psychotic disorder and treat with an appropriate algorithm for that. So if they have psychosis, sometimes it will remit with an SSRI. If not, we recommend adding an antipsychotic.
Slide 14 of 14
Risperidone has the best evidence in that, it had a clear-cut randomized controlled trial focusing on this subpopulation exclusively. Quetiapine had an RCT with a more mixed population. Aripiprazole has fewer side effects, seems to probably work so we do favor it as the first antipsychotic to try for this point in the algorithm.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
