
Slides and Transcript
Slide 1 of 10
We continue this presentation of an algorithm for the psychopharm treatment of PTSD and in this section, we’re going to talk about the management of sleep initiation disturbances in PTSD, trouble falling asleep.
Slide 2 of 10
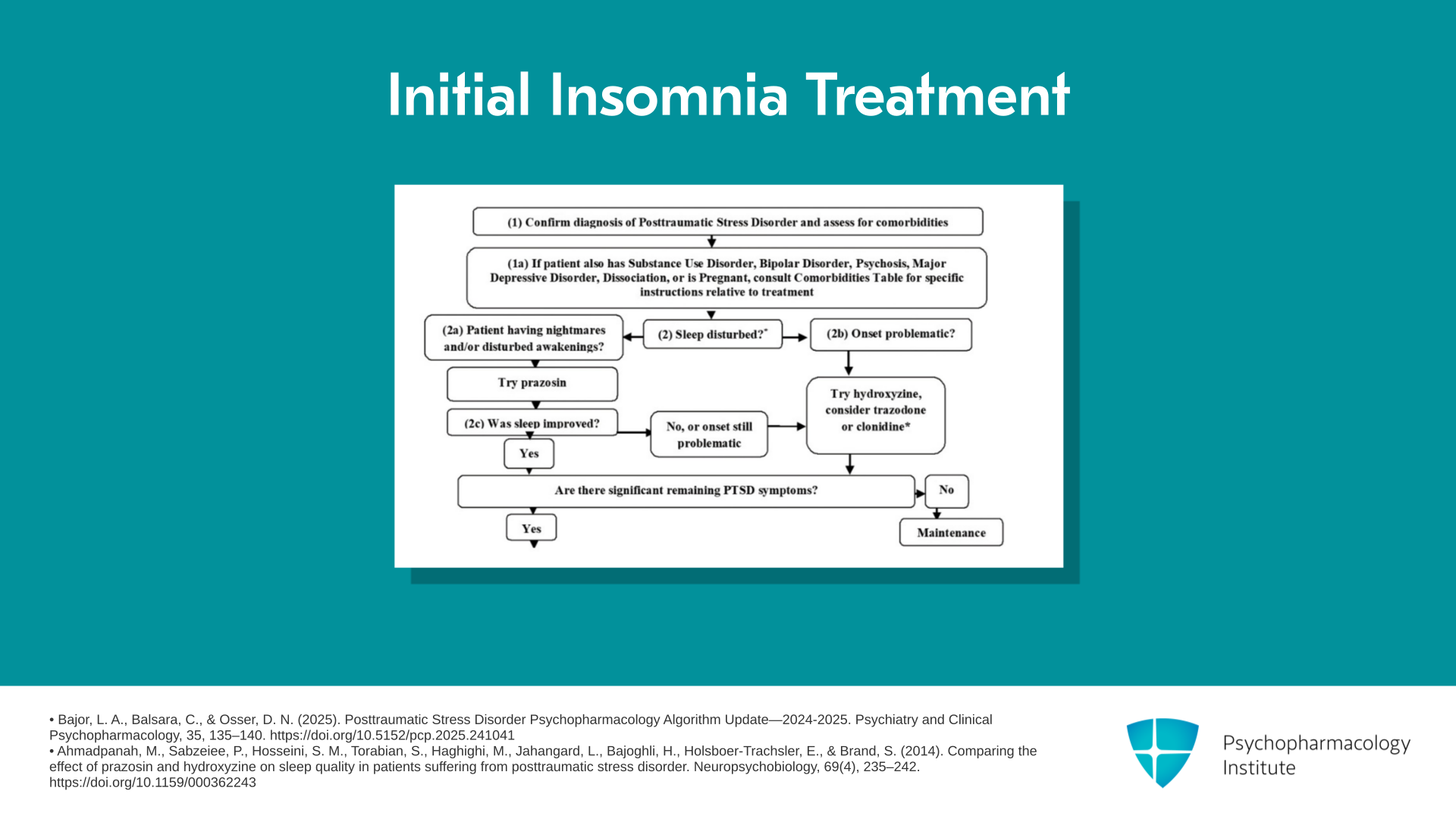
So as you can see on the flow chart, we’re at the point where you have someone who can’t fall asleep. Now, they may have gotten there because that’s their main problem or they may have gotten there because you treated their trouble staying asleep but they still have trouble falling asleep. So what do we recommend? We consider hydroxyzine our first line with trazodone a second line. And if prazosin worked for the nightmares and disturbed awakenings but initial insomnia is still present, again, hydroxyzine first, trazodone second. But we do have case series data on clonidine that make us want to consider it.
References:
- Bajor, L. A., Balsara, C., & Osser, D. N. (2025). Posttraumatic Stress Disorder Psychopharmacology Algorithm Update—2024-2025. Psychiatry and Clinical Psychopharmacology, 35, 135–140. https://doi.org/10.5152/pcp.2025.241041
- Ahmadpanah, M., Sabzeiee, P., Hosseini, S. M., Torabian, S., Haghighi, M., Jahangard, L., Bajoghli, H., Holsboer-Trachsler, E., & Brand, S. (2014). Comparing the effect of prazosin and hydroxyzine on sleep quality in patients suffering from posttraumatic stress disorder. Neuropsychobiology, 69(4), 235–242. https://doi.org/10.1159/000362243
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 10
This was a case series, retrospective chart review of 79 veterans in Chicago in a VA that were put on clonidine for their sleep problems due to PTSD. Looking at their CGI, Clinical Global Impression of Improvement, retrospectively in the chart review, it looked like 72% had met the criteria for improvement. They were either much improved or very much improved by the CGI. Whereas, there was no placebo control unfortunately. So we don’t know how placebo would’ve done. There were also minimum side effects reported.
References:
- Burek, G. A., Waite, M. R., Heslin, K., Liewen, A. K., Yaqub, T. M., & Larsen, S. E. (2021). Low-dose clonidine in veterans with posttraumatic stress disorder. Journal of Psychiatric Research, 137, 480–485. https://doi.org/10.1016/j.jpsychires.2021.03.008
Slide 4 of 10
Now, I know that there’s a lot of clinicians out there that are using it now before prazosin. It’s got zero controlled studies. Why would you use that first when we have something with 10 placebo-controlled trials of which 7 were positive. Furthermore, clonidine is a strong antihypertensive, much stronger than prazosin. So you’re going to be giving people more blood pressure problems than they need to have, and yet the drug has no evidence in the form of any placebo-controlled trials.
References:
- Burek, G. A., Waite, M. R., Heslin, K., Liewen, A. K., Yaqub, T. M., & Larsen, S. E. (2021). Low-dose clonidine in veterans with posttraumatic stress disorder. Journal of Psychiatric Research, 137, 480–485. https://doi.org/10.1016/j.jpsychires.2021.03.008
- Wendell, K. R., & Maxwell, M. L. (2015). Evaluation of clonidine and prazosin for the treatment of nighttime posttraumatic stress disorder symptoms. Federal Practitioner, 32(11), 8-14.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 10
The suggested dose of clonidine from the Burek retrospective experience-based data is 0.1 mg to 0.2 mg at bedtime which I understand he raises up to as high as 0.5 mg if tolerated. And then he also gives some in the daytime in their clinic, 0.05, in other words half of a 0.1 mg tablet up to three times a day as needed for PTSD day symptoms.
References:
- Burek, G. A., Waite, M. R., Heslin, K., Liewen, A. K., Yaqub, T. M., & Larsen, S. E. (2021). Low-dose clonidine in veterans with posttraumatic stress disorder. Journal of Psychiatric Research, 137, 480–485. https://doi.org/10.1016/j.jpsychires.2021.03.008
Slide 6 of 10
And there have been some clinicians there that have tried the clonidine patch to give them more control of the input of the clonidine during the course of the day. The experience of Burek is that it is helpful for falling asleep unlike prazosin seems to be as well as maintaining them.
References:
- Burek, G. A., Waite, M. R., Heslin, K., Liewen, A. K., Yaqub, T. M., & Larsen, S. E. (2021). Low-dose clonidine in veterans with posttraumatic stress disorder. Journal of Psychiatric Research, 137, 480–485. https://doi.org/10.1016/j.jpsychires.2021.03.008
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 10
So that concludes this short section on the alternatives for treating sleep. Be sure you’ve assessed the multiple other causes of difficulty falling asleep. One of which is conditioned insomnia. Conditioned insomnia is when you once had something causing you great difficulty sleeping like nightmares, so you’re afraid to sleep or you’re just afraid even without it being a nightmare, just the whole experience of tossing and turning. It can be a trauma, even though we’ve fixed what caused it, you’re still worried that you won’t fall asleep and you’ll be looking at the clock. Gee whiz, what time is it now? Oh, it’s now 1 o’clock. I got to get up for work. Oh no, now, it’s 1:30. So you’re worrying. This is called conditioned insomnia.
References:
- Bajor, L. A., Balsara, C., & Osser, D. N. (2025). Posttraumatic Stress Disorder Psychopharmacology Algorithm Update—2024-2025. Psychiatry and Clinical Psychopharmacology, 35, 135–140. https://doi.org/10.5152/pcp.2025.241041
- Kanady, J. C., Talbot, L. S., Maguen, S., Straus, L. D., Richards, A., Ruoff, L., & Neylan, T. C. (2018). Cognitive behavioral therapy for insomnia reduces fear of sleep in individuals with posttraumatic stress disorder. Journal of Clinical Sleep Medicine, 14(7), 1177–1188. https://doi.org/10.5664/jcsm.7224
Slide 8 of 10
The best treatment for that is cognitive behavioral therapy for insomnia, CBT-I, where you teach the patient how to think of other more relaxing things than these worries that they won’t be able to fall asleep.
References:
- Bajor, L. A., Balsara, C., & Osser, D. N. (2025). Posttraumatic Stress Disorder Psychopharmacology Algorithm Update—2024-2025. Psychiatry and Clinical Psychopharmacology, 35, 135–140. https://doi.org/10.5152/pcp.2025.241041
- Kanady, J. C., Talbot, L. S., Maguen, S., Straus, L. D., Richards, A., Ruoff, L., & Neylan, T. C. (2018). Cognitive behavioral therapy for insomnia reduces fear of sleep in individuals with posttraumatic stress disorder. Journal of Clinical Sleep Medicine, 14(7), 1177–1188. https://doi.org/10.5664/jcsm.7224
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 9 of 10
The key points are: In this short meeting, we covered problems with falling asleep. That may be the main problem or it could be a residual problem after you have successfully treated problems staying asleep with prazosin because prazosin is not sedating and has minimal benefit for falling asleep. So what do you use though for falling asleep? Given that we prefer to employ meds that have the best evidence or some evidence at least like we do in all our algorithms, that’s why we picked hydroxyzine. And after that, we suggest trazodone which has essentially no significant study in PTSD but is very widely used. It does seem to help people fall asleep. It does not usually help though with nightmares and disturbed awakenings.
Slide 10 of 10
Then I talked about clonidine as a promising option that’s more sedating than prazosin and probably helps people fall asleep better. And I have already described the published series of 79 patients given clonidine where 49% were rated as much or very much improved on the CGI.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
