Slides and Transcript
Slide 1 of 21
In this section, I’m going to talk about mood stabilizers in hemodialysis.
Slide 2 of 21
Lithium first of all. Lithium probably presents the most complex management scenario in terms of psychiatric drugs in dialysis, and that’s because it is entirely renally cleared and it is also removed by the process of dialysis. It is not impossible, however, to use lithium in patients who are undergoing dialysis with some careful planning.
References:
- Lambert, C. G., McWilliams, S., O'Donoghue, B., et al. (2021). Concurrent lithium and haemodialysis treatment: Clinical recommendations based on the literature and a multicentre survey. Bipolar Disorders, 23(7), 733–744. https://doi.org/10.1111/bdi.13390
- Bjarnason, N. H., Munkner, R., Kampmann, J. P., Tornoe, C. W., Ladefoged, S., & Dalhoff, K. (2006). Optimizing lithium dosing in hemodialysis. Therapeutic Drug Monitoring, 28(2), 262–266. https://doi.org/10.1097/01.ftd.0000183386.35018.86
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 21
Lithium has a two-compartment pharmacokinetic model. Lithium is initially distributed to the extracellular space and then it gradually moves into the intracellular space. And it takes about 5 to 10 days for that equilibration to occur. So it moves between the intracellular and the extracellular space. Now, lithium can only be removed by dialysis from the extracellular space and so that means that when it’s removed by dialysis, the equilibrium slowly returns over about 5 to 10 days with lithium then moving out of the intracellular space. So you, in fact, get an increased plasma concentration, a rebound after dialysis.
References:
- Lambert, C. G., McWilliams, S., O'Donoghue, B., et al. (2021). Concurrent lithium and haemodialysis treatment: Clinical recommendations based on the literature and a multicentre survey. Bipolar Disorders, 23(7), 733–744. https://doi.org/10.1111/bdi.13390
- Bjarnason, N. H., Munkner, R., Kampmann, J. P., Tornoe, C. W., Ladefoged, S., & Dalhoff, K. (2006). Optimizing lithium dosing in hemodialysis. Therapeutic Drug Monitoring, 28(2), 262–266. https://doi.org/10.1097/01.ftd.0000183386.35018.86
Slide 4 of 21
So what we’re aiming for if we give lithium to a patient who is undergoing dialysis bearing in mind that this process of dialysis will almost entirely remove lithium from the patient is for a stable therapeutic plasma concentration of lithium between dialysis sessions. And in order to achieve that, it’s usually necessary to give the patient a single dose of lithium immediately after the dialysis finishes and then nothing else until the next dialysis session. So that single dose of lithium is going to stay in the body until the next dialysis session when it’s going to be removed by the dialysis. So just as a reminder, that’s because lithium is entirely renally cleared. So if you have a patient who has no renal function and that’s why they’re undergoing dialysis, then the lithium won’t go anywhere until the next dialysis session.
References:
- Lambert, C. G., McWilliams, S., O'Donoghue, B., et al. (2021). Concurrent lithium and haemodialysis treatment: Clinical recommendations based on the literature and a multicentre survey. Bipolar Disorders, 23(7), 733–744. https://doi.org/10.1111/bdi.13390
- Bjarnason, N. H., Munkner, R., Kampmann, J. P., Tornoe, C. W., Ladefoged, S., & Dalhoff, K. (2006). Optimizing lithium dosing in hemodialysis. Therapeutic Drug Monitoring, 28(2), 262–266. https://doi.org/10.1097/01.ftd.0000183386.35018.86
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 21
Now, if you have a patient who has significant residual diuresis present, then you might find that it is necessary to do some form of daily dosing of the lithium for that patient but it’s likely to be a much smaller dose.
References:
- Bjarnason, N. H., Munkner, R., Kampmann, J. P., Tornoe, C. W., Ladefoged, S., & Dalhoff, K. (2006). Optimizing lithium dosing in hemodialysis. Therapeutic Drug Monitoring, 28(2), 262–266. https://doi.org/10.1097/01.ftd.0000183386.35018.86
Slide 6 of 21
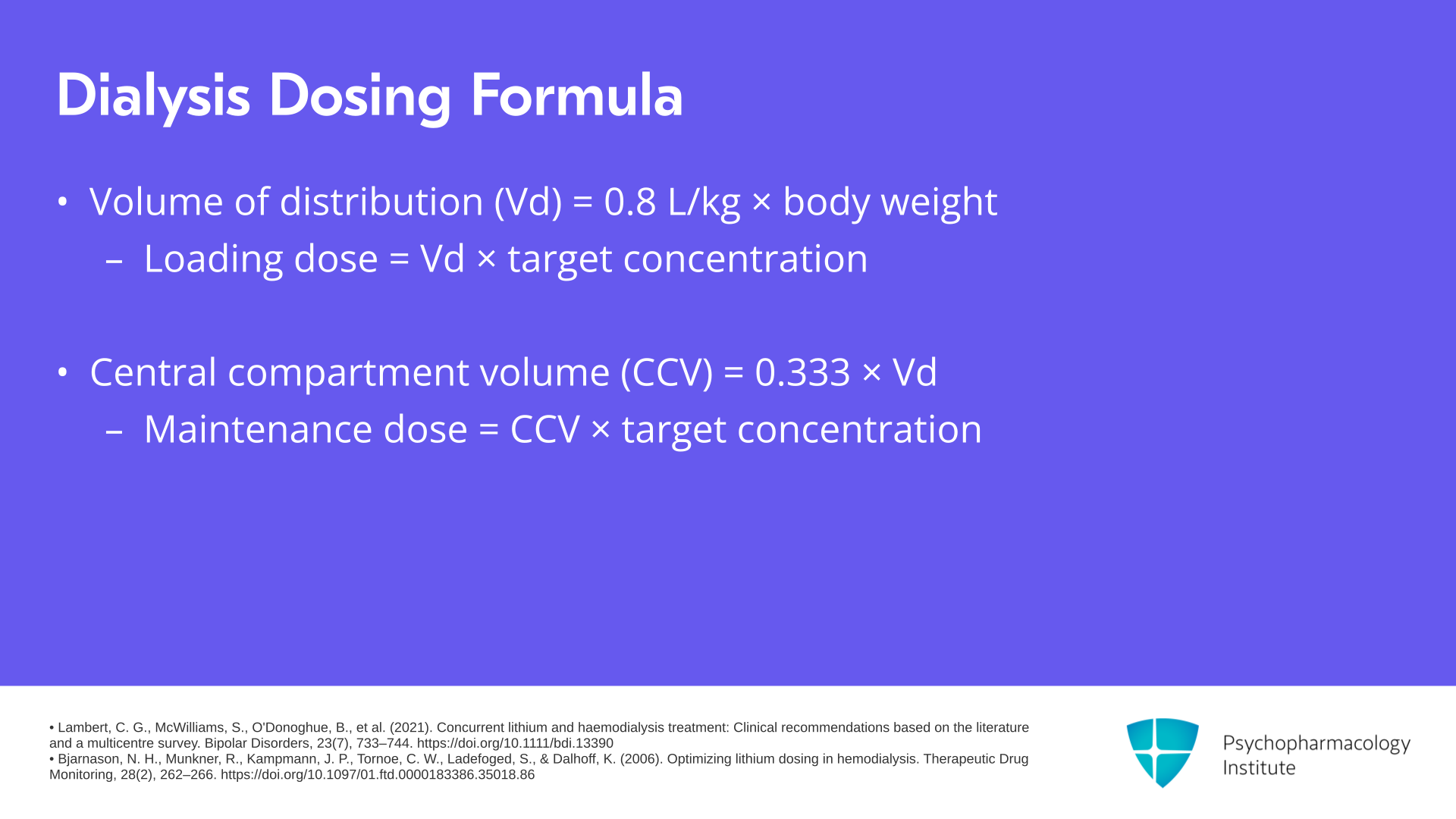
In terms of how to work out what dose to give a patient who’s undergoing dialysis, there are various ways of doing this. There’s one group who have created a formula for it which involves using the volume of distribution which is 0.8 L/kg times body weight of the patient to work out the volume of distribution for lithium for that individual patient. You can then work out a loading dose of lithium so that’s the volume of distribution multiplied by the target concentration and that’s the dose that you would then give once after the first dialysis session. You then work out the central compartment volume for the patient which is 0.333 times the volume of distribution and use that to calculate a maintenance dose which is the central compartment volume multiplied by the target concentration. And that’s then the dose you give after subsequent dialysis sessions.
References:
- Lambert, C. G., McWilliams, S., O'Donoghue, B., et al. (2021). Concurrent lithium and haemodialysis treatment: Clinical recommendations based on the literature and a multicentre survey. Bipolar Disorders, 23(7), 733–744. https://doi.org/10.1111/bdi.13390
- Bjarnason, N. H., Munkner, R., Kampmann, J. P., Tornoe, C. W., Ladefoged, S., & Dalhoff, K. (2006). Optimizing lithium dosing in hemodialysis. Therapeutic Drug Monitoring, 28(2), 262–266. https://doi.org/10.1097/01.ftd.0000183386.35018.86
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 21
An alternative way is to just take a cautious approach. Most authors start with 200 or perhaps 400 mg just once after the dialysis session. You then don’t give any doses of lithium on the non-dialysis days. Take plasma concentrations. Ideally, I think you want to be doing them daily and then you adjust doses in accordance with plasma concentrations.
References:
- Topp, S., & Salisbury, E. (2021). Lithium use in a patient on haemodialysis with bipolar affective disorder and lithium-induced nephropathy. BMJ Case Reports, 14(7), e242841. https://doi.org/10.1136/bcr-2021-242841
- McGrane, I. R., Omar, F. A., Morgan, N. F., & Shuman, M. D. (2022). Lithium therapy in patients on dialysis: A systematic review. The International Journal of Psychiatry in Medicine, 57(3), 187–201. https://doi.org/10.1177/00912174211030408
Slide 8 of 21
Special considerations for some patients. So if you have a patient who requires a very long dialysis session, more than five hours for example, they may need a higher dose because you’re expecting more lithium will be cleared. The hematocrit of an individual patient also affects the removal of lithium. So some lithium partitions into platelets and so the lower the hematocrit of the patient, the higher the clearance of lithium will be by dialysis because there is more lithium available in the blood to be cleared.
References:
- Lambert, C. G., McWilliams, S., O'Donoghue, B., et al. (2021). Concurrent lithium and haemodialysis treatment: Clinical recommendations based on the literature and a multicentre survey. Bipolar Disorders, 23(7), 733–744. https://doi.org/10.1111/bdi.13390
- Olyaei, A. J., & Steffl, J. L. (2011). A quantitative approach to drug dosing in chronic kidney disease. *Blood Purification*, *31*(1-3), 138–145. https://doi.org/10.1159/000321857
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 9 of 21
And residual diuresis as I mentioned earlier, but also sweat can remove lithium. So if you have a patient who had a lot of residual diuresis or sweating, then in theory they may require a higher lithium dose because more of it will be removed in between dialysis sessions by those processes.
References:
- Lambert, C. G., McWilliams, S., O'Donoghue, B., et al. (2021). Concurrent lithium and haemodialysis treatment: Clinical recommendations based on the literature and a multicentre survey. Bipolar Disorders, 23(7), 733–744. https://doi.org/10.1111/bdi.13390
- Olyaei, A. J., & Steffl, J. L. (2011). A quantitative approach to drug dosing in chronic kidney disease. *Blood Purification*, *31*(1-3), 138–145. https://doi.org/10.1159/000321857
Slide 10 of 21
Monitoring is going to be key, and daily pre-dialysis plasma concentrations are going to be necessary for at least the first two weeks when managing lithium in a patient undergoing hemodialysis. You want to look at a pre-dialysis concentration, because you want to know what the lithium level is before the dialysis session starts and you want that to be in the therapeutic range. It would be wise to aim for the lower end of the therapeutic range at least initially and that accounts for the heightened sensitivity and blood-brain barrier permeability in uremia for patients with chronic kidney disease. So you would expect an increased risk of adverse effects.
References:
- Bjarnason, N. H., Munkner, R., Kampmann, J. P., Tornoe, C. W., Ladefoged, S., & Dalhoff, K. (2006). Optimizing lithium dosing in hemodialysis. Therapeutic Drug Monitoring, 28(2), 262–266. https://doi.org/10.1097/01.ftd.0000183386.35018.86
- Chang, C. W. L., & Ho, C. S. H. (2020). Lithium use in a patient with bipolar disorder and end-stage kidney disease on hemodialysis: A case report. *Frontiers in Psychiatry*, *11*, 6. https://doi.org/10.3389/fpsyt.2020.00006
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 11 of 21
Once you’ve identified a maintenance dose for the lithium that is suitable for that patient, you could reduce the frequency of monitoring of the plasma concentration to dialysis days only. And once you’ve achieved stability which I would say is three consecutive stable concentrations of lithium, you could probably extend the plasma concentration monitoring to one to three times a month. That will need to be in conjunction though with careful observation for toxicity or signs of relapse.
References:
- Lambert, C. G., McWilliams, S., O'Donoghue, B., et al. (2021). Concurrent lithium and haemodialysis treatment: Clinical recommendations based on the literature and a multicentre survey. Bipolar Disorders, 23(7), 733–744. https://doi.org/10.1111/bdi.13390
- Olyaei, A. J., & Steffl, J. L. (2011). A quantitative approach to drug dosing in chronic kidney disease. *Blood Purification*, *31*(1-3), 138–145. https://doi.org/10.1159/000321857
Slide 12 of 21
Another tip is to make sure that you’re using the correct blood tubes. There are some blood tubes that have lithium heparin anticoagulant in them and that is going to affect the plasma concentration that you measure of the lithium of course.
References:
- Lambert, C. G., McWilliams, S., O'Donoghue, B., et al. (2021). Concurrent lithium and haemodialysis treatment: Clinical recommendations based on the literature and a multicentre survey. Bipolar Disorders, 23(7), 733–744. https://doi.org/10.1111/bdi.13390
- Olyaei, A. J., & Steffl, J. L. (2011). A quantitative approach to drug dosing in chronic kidney disease. *Blood Purification*, *31*(1-3), 138–145. https://doi.org/10.1159/000321857
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 13 of 21
Another consideration is the dialysate that is being used. It’s possible that bicarbonate-based solutions might remove lithium more efficiently than acetate-based solutions are, and that would result in less of the rebound effect that I mentioned earlier and possibly lower post-dialysis requirements for lithium dose. So if these things change in the process of the dialysis journey for that patient, then it would be worth making sure that extra monitoring is put in place.
References:
- Szerlip, H. M., Heeger, P., & Feldman, G. M. (1992). Comparison between acetate and bicarbonate dialysis for the treatment of lithium intoxication. American Journal of Nephrology, 12(1-2), 116–120. https://doi.org/10.1159/000168430
Slide 14 of 21
Moving on to talk about sodium valproate. It’s extensively metabolized by the liver but the metabolites are excreted by the kidneys and it has quite a low volume of distribution. It’s about 0.1 to 0.4 L/kg. Valproate is highly protein bound and that means that there’s the potential for an increased free fraction of valproate if the patient has low albumin. As a reminder, high protein binding of a drug makes dialysis quite unlikely except in the case of overdose, where you can saturate the binding of proteins. So for valproate, the free fraction is going to be quite important.
References:
- Kandrotas, R. J., Love, J. M., Gal, P., & Oles, K. S. (1990). The effect of hemodialysis and hemoperfusion on serum valproic acid concentration. *Neurology*, *40*(9), 1456–1458. https://doi.org/10.1212/wnl.40.9.1456
- Franssen, E. J., van Essen, G. G., Portman, A. T., de Jong, J., Go, G., Stegeman, C. A., & Uges, D. R. (1999). Valproic acid toxicokinetics: Serial hemodialysis and hemoperfusion. Therapeutic Drug Monitoring, 21(3), 289–292. https://doi.org/10.1097/00007691-199906000-00005
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 15 of 21
There are some case reports in terms of removal by dialysis that show no changes in valproate plasma concentration on days of dialysis which would indicate no removal by dialysis and no problem. But there are other studies that show about 20% dose removal by dialysis, 20% for low-efficiency dialysis and up to 42% in high-efficiency dialysis. So all of that is to say that it’s not entirely clear what the effect of dialysis will be on sodium valproate. And it’s going to be important to measure plasma concentrations pre and post dialysis to determine if any extra doses are needed, because it’s not possible to predict exactly how much of the dose will be removed by dialysis.
References:
- Araki, K., Nakamura, T., Takeuchi, Y., Morozumi, S., Horie, K., Kobayashi, Y., Kawakami, O., Sobue, F., Ueda, T., Hamada, K., Ando, T., Inoue, Y., Yasui, K., Morozumi, K., Maruyama, S., & Katsuno, M. (2020). Pharmacological monitoring of antiepileptic drugs in epilepsy patients on haemodialysis. Epileptic Disorders, 22(1), 90–102. https://doi.org/10.1684/epd.2020.1139
- Kandrotas, R. J., Love, J. M., Gal, P., & Oles, K. S. (1990). The effect of hemodialysis and hemoperfusion on serum valproic acid concentration. *Neurology*, *40*(9), 1456–1458. https://doi.org/10.1212/wnl.40.9.1456
Slide 16 of 21
A simple solution might be simply to give the dose after the dialysis has finished. But bear in mind that uremia on the non-dialysis days might increase the free drug proportion of valproate. And so if adverse effects start to appear between dialysis sessions, it may be worth checking a plasma concentration of valproate. For psychiatric indications though, there tends to be little consequence to small transient changes in plasma concentration at least in terms of efficacy.
References:
- Dasgupta, A., Jacques, M., & Malhotra, D. (1996). Diminished protein binding capacity of uremic sera for valproate following hemodialysis: role of free fatty acids and uremic compounds. American Journal of Nephrology, 16(4), 327–333. https://doi.org/10.1159/000169018
- Kandrotas, R. J., Love, J. M., Gal, P., & Oles, K. S. (1990). The effect of hemodialysis and hemoperfusion on serum valproic acid concentration. *Neurology*, *40*(9), 1456–1458. https://doi.org/10.1212/wnl.40.9.1456
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 17 of 21
Lamotrigine is primarily hepatically metabolized by glucuronidation and the glucuronide metabolite of lamotrigine is excreted via the kidneys. But the metabolite is inactive and so impaired excretion of it doesn’t affect the parent drug plasma concentration. Dosing alterations therefore for renal impairment shouldn’t be necessary, although the manufacturers of lamotrigine advise caution because of the unknown consequences of metabolite accumulation.
References:
- Araki, K., Nakamura, T., Takeuchi, Y., Morozumi, S., Horie, K., Kobayashi, Y., Kawakami, O., Sobue, F., Ueda, T., Hamada, K., Ando, T., Inoue, Y., Yasui, K., Morozumi, K., Maruyama, S., & Katsuno, M. (2020). Pharmacological monitoring of antiepileptic drugs in epilepsy patients on haemodialysis. Epileptic Disorders, 22(1), 90–102. https://doi.org/10.1684/epd.2020.1139
- Betchel, N. T., Fariba, K. A., & Saadabadi, A. (2023). Lamotrigine. In *StatPearls* [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK470442/
Slide 18 of 21
There’s disagreement in the literature about the dialyzability of lamotrigine. Some sources state that it’s not removed by dialysis but it has a very low volume of distribution. It’s about 0.9 to 1.2 L/kg, and it is about 55% protein bound. So as for valproate, it would be wise to monitor plasma concentrations and monitor the patient carefully for any emergent adverse effects or relapse.
References:
- Araki, K., Nakamura, T., Takeuchi, Y., Morozumi, S., Horie, K., Kobayashi, Y., Kawakami, O., Sobue, F., Ueda, T., Hamada, K., Ando, T., Inoue, Y., Yasui, K., Morozumi, K., Maruyama, S., & Katsuno, M. (2020). Pharmacological monitoring of antiepileptic drugs in epilepsy patients on haemodialysis. Epileptic Disorders, 22(1), 90–102. https://doi.org/10.1684/epd.2020.1139
- Betchel, N. T., Fariba, K. A., & Saadabadi, A. (2023). Lamotrigine. In *StatPearls* [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK470442/
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 19 of 21
Key points then for the use of mood stabilizers in patients with hemodialysis. Lithium is almost entirely renally cleared, and it is removed by the process of dialysis. Use of it should therefore be avoided if that’s possible, but if it is essential to continue lithium, the simplest solution is to give a single dose of lithium after the dialysis and then not give it again until the next dialysis session. Plasma concentrations of lithium pre-dialysis should be used to guide dosing. Initial doses should be started cautiously at 200 mg or calculated using pharmacokinetic principles.
Slide 20 of 21
The metabolites of sodium valproate are extensively renally cleared. It’s highly protein bound and so the free fraction of valproate may increase in low albumin states such as end-stage renal failure. It’s unclear to what extent sodium valproate is dialyzed. Give the dose after dialysis and monitor plasma concentrations.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 21 of 21
Lamotrigine is hepatically cleared. Dose adjustment should therefore be unnecessary in renal impairment although there may be accumulation of the metabolically inactive metabolite. It’s not clear whether lamotrigine is dialyzed or not. Give the dose after dialysis and monitor plasma concentrations.