
Text Version
Dosing in Schizophrenia
Flavio Guzman, M.D.: Dr. Kane, how has your view of adequate dosing in schizophrenia changed over your career? Was there a finding that made you rethink it?
John Kane, M.D.: Many patients with schizophrenia during the initial episode respond well to antipsychotic medication. There is a place for therapeutic drug monitoring in establishing the best dose for each patient, but it is not widely used except in the case of clozapine.
Over the years, we have also learned that some patients respond to lower doses than originally anticipated — both in acute treatment and in maintenance treatment. Titrating the dose remains an individual challenge.
The introduction of medications that are better tolerated in terms of neurologic side effects has also expanded the opportunity to adjust dosing in ways that were more limited with some first-generation agents.
One of the biggest challenges is determining what to do when a patient does not respond to what appears to be an adequate dose. The key questions become:
- Is the patient actually taking the medication?
- Is the patient absorbing and metabolizing the medication in an unusual way?
This is where therapeutic drug monitoring plays an important role. There is not strong evidence that increasing doses outside the therapeutic range improves efficacy, nor that switching from one medication to another — apart from clozapine — is likely to produce added benefit.
Clozapine plays an important role in the management of treatment-resistant patients. In my opinion, we need to take better advantage of therapeutic drug monitoring to determine whether a patient has a therapeutic plasma level, which provides very important clinical information.
Download PDF and other files
TDM: Biggest Obstacle to Routine Practice
Flavio Guzman, M.D.: What are the biggest obstacles to TDM becoming routine in psychiatry? And what would actually help change that?
John Kane, M.D.: It is something of a catch-22. We do not have enough data on therapeutic ranges for some medications, which may discourage clinicians — but if clinicians are not requesting more data to inform their practice, that data is unlikely to be generated.
Availability is also a significant barrier. Point-of-care tools would be very valuable. Clinicians are currently discouraged by the fact that results may take many days or even weeks to return, depending on the institution and the laboratory’s capabilities.
There are a number of contributing factors, but if one had to be identified above all others, it is this: therapeutic drug monitoring is not viewed as part of routine clinical practice.
TDM Sampling: Timing and Common Mistakes
Flavio Guzman, M.D.: Let’s talk about sampling. When can you trust a level, and when does timing make it hard to interpret? What mistakes do you see most often?
John Kane, M.D.: Levels should generally be obtained 12 hours after the last dose. Deviating significantly from that window makes the result difficult to interpret.2
Another common mistake is placing too much weight on a single level. When a level raises clinical concern, it should be repeated — especially when an important clinical decision depends on it.
Plasma levels can fluctuate even under normal circumstances. With clozapine, for example, variation of 20 to 30 percent from one assay to the next is not unusual.1
It is important to use the same laboratory consistently, one with rigorous quality assessment. Key considerations for reliable sampling include:
- Timing the draw 12 hours after the last dose (the relative trough for oral medications)
- Waiting until the patient has achieved steady state — typically five half-lives of the medication 2
- For long-acting injectable medications: drawing the level just before the next injection, or up to 48 to 72 hours before, to assess the trough
The most common errors are incorrect timing, over-reliance on a single unrepeated level, and drawing levels before steady state is achieved.
Download PDF and other files
Treatment-Resistant Schizophrenia
Flavio Guzman, M.D.: After decades with treatment-resistant patients, what is the most common reason a patient is wrongly labeled treatment resistant — the so-called pseudo-resistance? And how do you spot it?
John Kane, M.D.: The most common reason patients are identified as treatment-resistant when they are not is subtherapeutic or undetectable plasma levels. Before considering someone treatment-resistant, it is essential to confirm that they have actually been taking the medication as prescribed.
This requires either therapeutic drug monitoring or a trial of a long-acting injectable antipsychotic. A long-acting injectable trial typically requires approximately four months to achieve steady state and determine whether the patient will respond.
Therapeutic drug monitoring is a particularly valuable tool for establishing whether the patient was receiving a therapeutic dose of each medication they are reported to have failed.1 We do not want to mislabel a patient as treatment-resistant when the true issue is non-adherence — that is a critical clinical distinction.
Clozapine TDM Algorithm
Flavio Guzman, M.D.: Clozapine is the only antipsychotic with its own TDM algorithm. For someone who does not use it often, can you walk us through it — from subtherapeutic to in-range, supratherapeutic, and the alert threshold?
John Kane, M.D.: Clozapine is a medication with special considerations — it is the only agent indicated for treatment-resistant schizophrenia and carries an FDA indication for suicidality as well. It has a range of adverse effects, and fortunately there is a meaningful body of data to help identify therapeutic thresholds.
Clozapine should be titrated slowly. The pace may be somewhat faster for inpatients than for outpatients:
- Inpatients: may reach 200 mg within approximately 16 days
- Outpatients: a more gradual approach, reaching 200 mg after approximately 24 days
When the patient reaches 100 mg or 200 mg, many recommend waiting five to seven days and then obtaining a plasma clozapine level — ideally 12 hours after the last dose. Because clozapine is typically dosed once daily at bedtime, a 12-hour post-dose draw is appropriate.
Guidelines generally place 350 ng/mL as the therapeutic threshold, though some patients respond at lower levels.
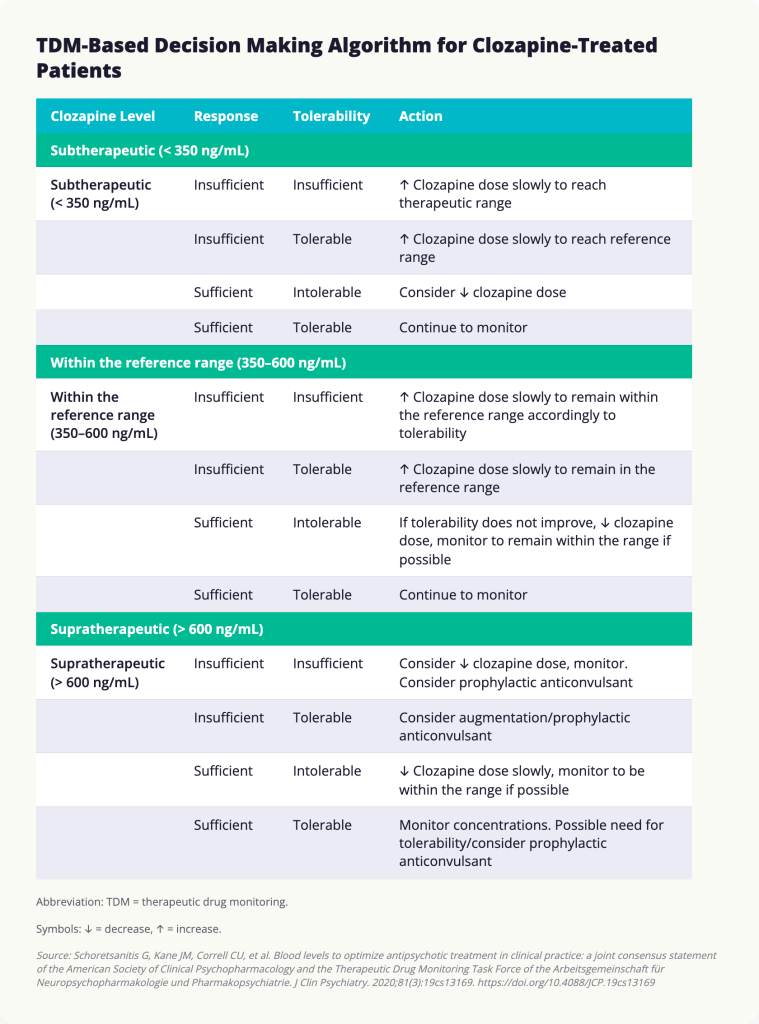
3 Clinical assessment must always guide interpretation:
- Observe how the patient is responding
- Evaluate whether expected therapeutic benefit is occurring
- Assess for adverse effects
These clinical observations ultimately determine the dose prescribed; therapeutic drug monitoring provides important ancillary information.
Smoking status is critical to know. Smoking as few as 7 to 12 cigarettes per day can fully induce CYP1A enzymes, significantly lowering clozapine levels. If a patient stops smoking, plasma levels may increase by as much as 50 percent, typically within seven to eight days of cessation.4
Infection or inflammation can also affect clozapine plasma levels.5 Regarding an upper threshold for concern, some have proposed 1,000 ng/mL as a potentially toxic level, though there are patients who tolerate this level without clinical difficulty.
At higher plasma levels, the following adverse effects are more likely and should be monitored:
- Sedation
- Orthostatic hypotension
- Tachycardia
- Sialorrhea
Regarding norclozapine, the active metabolite: current evidence does not support basing clinical decisions on the norclozapine level or the clozapine-to-norclozapine ratio alone. The ratio can reflect CYP1A activity — a significant change may indicate a new inhibitor or inducer of CYP1A has been introduced — but beyond that, the role of norclozapine measurement remains limited.
Download PDF and other files
Clozapine and Smoking Cessation
Flavio Guzman, M.D.: A patient on clozapine stops smoking. What happens to the level, how fast, and what is the right response?
John Kane, M.D.: Smoking has a significant and clinically meaningful impact on clozapine levels. As few as 7 to 12 cigarettes per day can fully induce the CYP1A enzyme, substantially lowering clozapine plasma concentrations.
When a patient stops smoking, plasma levels can increase by as much as 50 percent. This rise typically occurs over seven to eight days as the enzyme returns to baseline.
Patients and their families should be warned about the impact that smoking or smoking cessation can have on clozapine plasma levels. It is equally important that they understand infection can also influence levels — if a patient is admitted to the hospital with inflammation or infectious illness, a clozapine plasma level should be obtained.5
Clozapine-to-Norclozapine Ratio
Flavio Guzman, M.D.: In your experience, what does the clozapine-to-norclozapine ratio tell you that is most useful? And how is it commonly misread?
John Kane, M.D.: There has been considerable misconception about this ratio. Its most useful application is as a marker of CYP1A activity — a meaningful change in the ratio may indicate that a concomitant medication has been added or removed that inhibits or induces CYP1A. Beyond that signal, the ratio does not have a well-established role in routine clinical management.
Download PDF and other files
References
- Schoretsanitis G, Kane JM, Correll CU, et al. Blood Levels to Optimize Antipsychotic Treatment in Clinical Practice: A Joint Consensus Statement of the American Society of Clinical Psychopharmacology and the Therapeutic Drug Monitoring Task Force of the Arbeitsgemeinschaft für Neuropsychopharmakologie und Pharmakopsychiatrie. J Clin Psychiatry. 2020;81(3):19cs13169. https://doi.org/10.4088/JCP.19cs13169
- Hiemke C, Bergemann N, Clement HW, et al. Consensus Guidelines for Therapeutic Drug Monitoring in Neuropsychopharmacology: Update 2017. Pharmacopsychiatry. 2018;51(1-2):9-62. https://doi.org/10.1055/s-0043-116492
- Northwood K, Pearson E, Arnautovska U, et al. Optimising plasma clozapine levels to improve treatment response: an individual patient data meta-analysis and receiver operating characteristic curve analysis. Br J Psychiatry. 2023;222(6):241-245. https://doi.org/10.1192/bjp.2023.27
- Wagner E, McMahon L, Falkai P, et al. Impact of smoking behavior on clozapine blood levels – a systematic review and meta-analysis. Acta Psychiatr Scand. 2020;142(6):456-466. https://doi.org/10.1111/acps.13228
- Clark SR, Warren NS, Kim G, et al. Elevated clozapine levels associated with infection: A systematic review. Schizophr Res. 2018;192:50-56. https://doi.org/10.1016/j.schres.2017.03.045
