
In a nutshell
Gepirone is the first FDA-approved selective 5-HT1A agonist for major depressive disorder in adults. Its distinguishing tolerability features are placebo-level sexual dysfunction and weight neutrality. The trade-offs are ECG monitoring for QTc prolongation, a strict food requirement, and contraindication with strong CYP3A4 inhibitors. Efficacy is modest and was contested at the FDA before approval [1].

- When to consider gepirone:
- Gepirone has a narrow role, best considered as an alternative after SSRI/SNRI failure or intolerance [2,3]
- Bupropion is the closest non-serotonergic comparator (also weight-neutral, no sexual side effects)
- Generally prefer bupropion, given its broader evidence base and simpler logistics
- Gepirone is an option when bupropion is contraindicated, not tolerated, or has failed
- Treatment-emergent sexual dysfunction on SSRIs or SNRIs, when switching is preferred over augmentation
- Gepirone shows placebo-equivalent rates and may improve desire and arousal independent of mood improvement [4,5]
- Weight gain on prior antidepressants, or patients with metabolic risk factors [3]
- When bupropion is contraindicated, not tolerated, or has failed
- MDD with prominent anxious features, a weaker signal (subgroup analysis only) [6]
- Weigh against the ECG/food/CYP3A4 burden and standard options (SSRI/SNRI ± augmentation)
- Gepirone has a narrow role, best considered as an alternative after SSRI/SNRI failure or intolerance [2,3]
- Consider alternatives when:
- Baseline QTc > 450 msec, congenital long QT syndrome, or concurrent QT-prolonging medications [2,7]
- Concurrent strong CYP3A4 inhibitors (e.g., ketoconazole, clarithromycin, ritonavir): contraindicated
- Severe hepatic impairment, Child-Pugh C: contraindicated
- Patients unable to take medication with food at the same time daily [2,7]
Pharmacodynamics and mechanism of action
- Gepirone is an azapirone, structurally related to buspirone but with greater 5-HT1A receptor selectivity [2,7]
- First FDA-approved drug positioned as a selective 5-HT1A receptor agonist for MDD [7,8]
- No clinically significant binding to SERT, NET, or DAT [2,3]
- No dopaminergic side effects (eg, prolactin elevation, extrapyramidal symptoms)

- Primary mechanism: selective 5-HT1A receptor agonism
- High affinity for 5-HT1A receptors and substantially lower affinity for 5-HT2A receptors [2,7]
- Biased agonist:
- Gepirone exhibits location-dependent intrinsic activity at 5-HT1A receptors, with different signaling at presynaptic versus postsynaptic sites [2,3]
- Presynaptic 5-HT1A autoreceptors (somatodendritic, dorsal and median raphe nuclei): full agonist

- Postsynaptic 5-HT1A heteroreceptors (hippocampus, neocortex, septum, amygdala, hypothalamus): partial agonist

- Gepirone’s effect on serotonergic transmission is time-dependent, mirroring the delayed-onset model that applies broadly to monoaminergic antidepressants [2,9]
- Acute administration: full agonism at autoreceptors transiently suppresses dorsal raphe serotonergic firing and reduces 5-HT release in projection areas
- Chronic administration (≈2–4 weeks): somatodendritic autoreceptors desensitize and downregulate, removing the negative-feedback “brake” on serotonergic neurons, leading to a sustained increase in 5-HT release in cortico-limbic projections
- Clinical implications:
- Antidepressant and anxiolytic effects without the broad serotonergic stimulation of SSRIs/SNRIs [2,3]
- Selective 5-HT1A targeting avoids activation of 5-HT2 and 5-HT3 receptors, accounting for the lower rates of nausea persistence, sexual dysfunction, and emotional blunting compared with SSRIs [2,4]
- Comparison with buspirone and other azapirones[2]
- Buspirone:
- Partial 5-HT1A agonism at both pre- and postsynaptic sites + moderate D2 affinity
- Narrower antidepressant activity; FDA-approved for anxiety only
- Tandospirone:
- Similar partial 5-HT1A agonism + short half-life
- Available primarily in Japan/China for anxiety and depression
- Perospirone:
- Partial 5-HT1A agonism + potent D2 and 5-HT2A antagonism
- Atypical antipsychotic profile
- Buspirone:
- Active metabolites
- 3’-OH-gepirone:
- 5-HT1A agonist that circulates at higher concentrations than the parent drug and contributes meaningfully to clinical activity [2,7]
- 1-PP (1-(2-pyrimidinyl)-piperazine):
- α2-adrenergic receptor antagonist; shared with buspirone [7]
- Increases firing of locus coeruleus noradrenergic neurons and disinhibits 5-HT release at terminals [2,3]
- May contribute to noradrenergic activation and stimulant-type adverse effects (eg, jitteriness, palpitations)
- 3’-OH-gepirone:
Pharmacokinetics and Drug Interactions
Metabolism
- Gepirone is extensively metabolized in the liver, primarily by CYP3A4 [7,10]
- Minor contribution from CYP2D6
- Both major active metabolites (3’-OH-gepirone and 1-PP) circulate at higher plasma concentrations than the parent drug
- Gepirone is not a clinically significant inhibitor or inducer of cytochrome enzymes or major drug transporters [7]
- Chronic administration is unlikely to alter the metabolism of other CYP-dependent drugs

Food Effect: Bioavailability Considerations
- Gepirone must be taken with food at the same time each day to maintain steady plasma concentrations and avoid peak–trough variability [7]
- Exposure increases significantly with food, in a dose-of-fat–dependent manner [3,7,11]
Half-life
- Terminal half-life: ~5 hours for parent gepirone; ~5.8 hours for the 1-PP metabolite [2,7]
- Linear pharmacokinetics across the approved dose range
Drug Interactions
Pharmacokinetic Interactions
- Gepirone levels markedly increased by:
- Strong CYP3A4 inhibitors
- Contraindicated [2,7,12]
- The contraindication is driven by cardiac risk: combined CYP3A4 inhibition + dose-dependent QT prolongation can be life-threatening
- Examples: ketoconazole, itraconazole, clarithromycin, ritonavir, lopinavir, voriconazole
- Moderate CYP3A4 inhibitors
- Reduce gepirone dose by 50% [2,7]
- Monitor ECG more frequently during co-administration
- Examples: erythromycin, diltiazem, verapamil, fluconazole
- Grapefruit juice
- Counsel patients specifically to avoid grapefruit and grapefruit juice; patients often do not consider it a “drug”
- Inhibits intestinal CYP3A4 with a highly variable magnitude, so standardized dose adjustment is not feasible
- Strong CYP3A4 inhibitors
- Gepirone levels markedly decreased by:
- Strong CYP3A4 inducers[2,7]
- Avoid; dose escalation cannot reasonably compensate
- Switch the inducer or select an alternative antidepressant
- Examples: rifampin, carbamazepine, phenytoin, phenobarbital, St. John’s Wort, enzalutamide, mitotane
- Rifampin 600 mg daily reduced gepirone Cmax ~20× and AUC ~29× — exposure becomes essentially subtherapeutic [7]
- Moderate CYP3A4 inducers
- Monitor for loss of antidepressant efficacy; consider an alternative agent if symptoms re-emerge
- Examples: efavirenz, etravirine, modafinil
- Strong CYP3A4 inducers[2,7]
- Effects of gepirone on other drugs:
- Gepirone is not a CYP inhibitor or inducer at clinical exposures [7]
- Warfarin:
- No significant change in INR, prothrombin values, or warfarin pharmacokinetics with gepirone co-administration
- Gepirone can be safely combined with warfarin from a PK standpoint, though shared QT considerations still apply [7]
Pharmacodynamic Interactions
- Monoamine oxidase inhibitors (MAOIs)[2,7]
- Contraindicated; risk of serotonin syndrome and hypertensive crisis.
- Allow a 14-day washout between stopping an MAOI and starting gepirone, and between stopping gepirone and starting an MAOI
- Remember that IV methylene blue is an often-overlooked MAOI
- Linezolid: per FDA labeling, concomitant use is contraindicated [13–16]
- Other serotonergic drugs
- Increased risk of serotonin syndrome; monitor closely [7]
- Examples: SSRIs, SNRIs, TCAs, triptans, fentanyl, lithium, tramadol, tryptophan, St. John’s wort
- QT-prolonging agents — caution; intensify ECG monitoring[7]
- Exercise caution and monitor ECG more frequently
- Correct hypokalemia and hypomagnesemia before initiating gepirone, particularly in patients on diuretics, glucocorticoids, or with a history of electrolyte disturbance [7]
Dosage forms
- Extended-release tablets:
- 18.2 mg (pink), 36.3 mg (off-white), 54.5 mg (yellow), 72.6 mg (red-brown)
- Each tablet contains gepirone equivalent to 20, 40, 60, or 80 mg of gepirone HCl
- Exxua (also available as Exxua Titration Pack)
- No generic available
- Formulation considerations:
- Take with food at approximately the same time each day to ensure adequate, consistent absorption [7]
- Swallow whole — do not split, crush, or chew (extended-release matrix)
- The Exxua Titration Pack is a starter kit containing the 18.2 mg, 36.3 mg, and 54.5 mg tablet strengths in a single calendar-style blister to facilitate the standard 14-day titration schedule
- Grapefruit juice should be avoided as it inhibits CYP3A4 and can significantly increase gepirone levels
Indications
FDA-Approved Indications
Major Depressive Disorder (MDD)
- Gepirone extended-release is FDA-approved for the treatment of MDD in adults [7]
- First antidepressant approved as a selective 5-HT1A receptor agonist [2,3,8]
- Approval came only after a contested, three-decade journey [1,2]
- The efficacy signal is weak:
- Only 2 of 13 trials were positive (3 were statistically inferior to fluoxetine or paroxetine)
- Pooled gepirone–placebo difference: −0.48 HAMD-17 points (not significant) — vs. ~2.5 points for 18 other antidepressants in an FDA meta-analysis [1]
- Rejected four times (1999–2007); a 2015 FDA advisory committee then voted 9–4 that efficacy was not demonstrated.
- What ultimately secured approval was a sponsor-initiated dispute-resolution process: senior FDA leaders overrode both the original review team and the advisory committee, accepting the sponsor’s argument that the 2 positive trials met the statutory “substantial evidence” standard.
- The efficacy question was effectively settled in 2016 [1]
- The wait until September 2023 then reflected added safety requirements (QT, abuse potential, sexual dysfunction), not efficacy concerns [1]
- The efficacy signal is weak:
- Clinical positioning
- Best viewed as a niche agent, not a first-line antidepressant: the efficacy signal is modest, and the ECG, food, and CYP3A4 requirements add management burden [2,7]
- Major MDD guidelines do not yet provide formal placement for gepirone
- Most reasonable as a second-line option after SSRI/SNRI nonresponse or intolerance, particularly in the following scenarios [3]:
- Sexual dysfunction limited prior therapy, and bupropion or mirtazapine are unsuitable
- Weight neutrality is a priority (no clinically significant weight gain vs. placebo in pivotal trials) [3,7]
- Comorbid anxiety symptoms are prominent (see Off-Label and Emerging Uses below) [2,6]
- Prefer alternatives when any of the following are present:
- Cardiac risk factors or QTc concerns
- Electrolyte abnormalities
- Unavoidable strong CYP3A4 interactions
- Severe hepatic impairment
- Unreliable food intake (gepirone’s bioavailability is food-dependent, so erratic eating yields erratic exposure)
- Dosing[7]
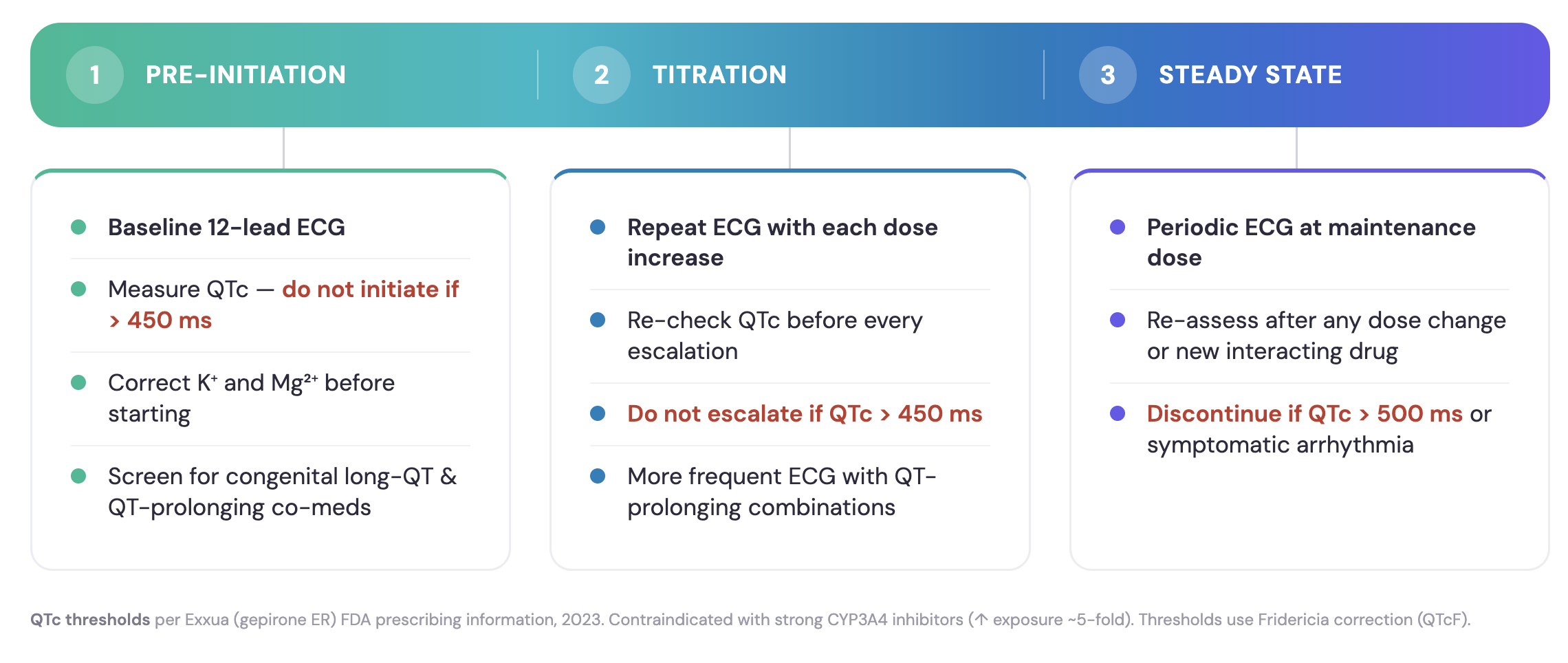
- Pre-treatment:
- Obtain baseline ECG and serum electrolytes
- Correct any hypokalemia or hypomagnesemia
- Do not initiate if QTc >450 msec
- Starting dose: 18.2 mg once daily with food
- Day 4: increase to 36.3 mg once daily
- After Day 7: increase to 54.5 mg once daily
- After Day 14: increase to 72.6 mg once daily (maximum dose)
- During treatment: repeat ECG with each dose escalation and periodically thereafter; do not escalate if QTc >450 msec
- Pre-treatment:
- Caveats and limitations
- Requires baseline ECG and ongoing QTc monitoring (do not initiate if QTc >450 msec)
- Must be taken with food at the same time each day; bioavailability and exposure are food-dependent [7]
- Strong CYP3A4 inhibitors are contraindicated; dose reductions are required with moderate inhibitors and in renal/hepatic impairment [3,7]
Off-Label and Emerging Uses
Sexual dysfunction associated with depression
- Unlike SSRIs, which characteristically worsen sexual function, gepirone may improve it.
- Improved hypoactive sexual desire disorder (HSDD) in depressed women across three RCTs, with benefit emerging by week 2 and sustained through week 8 [17]
- In men, sexual function improved even when depression did not respond, suggesting a pro-sexual effect at least partly independent of antidepressant action [5]
- Not FDA-approved for hypoactive sexual desire disorder; Phase III development for this indication has been discussed in the literature, but not carried to approval [2]
Anxiety disorders
- Not FDA-approved for anxiety disorders
- The IR formulation showed signals of anxiolytic activity in older studies of generalized anxiety disorder [2]
- A retrospective subgroup analysis of MDD trials suggested benefit in the anxious-depression subgroup, with significant improvement in the HAMD-17 anxiety/somatization factor [6]
- Plausible mechanistic rationale: 5-HT1A agonism produces anxiolytic as well as antidepressant effects, consistent with buspirone’s anxiolytic profile in GAD [2,3]
- Reasonable option in patients whose anxiety symptoms have been a barrier to tolerating activating SSRIs/SNRIs [2]
Side effects
Gepirone is generally well tolerated with respect to weight, sexual function, and sedation. It may produce dizziness in roughly half of patients, the leading cause of discontinuation. Nausea is also common but typically mild and self-limited.
The most relevant safety concern is dose-dependent QTc prolongation, which requires ECG monitoring. [2,7]
Most common side effects
Neurological/Psychiatric
- Dizziness (49% incidence; placebo 10%) [7]
- The most common adverse reaction and most frequent reason for discontinuation [3,7]
- Often described as lightheadedness, postural dizziness, or vertigo; typically emerges during titration and is dose-dependent [2,7]
- More common in male patients and in patients < 40 years of age [7]
- Clinical tips: take with food at the same time each day, advise patients to rise slowly from sitting/lying positions, and consider slowing titration if intolerable
- Headache (31%; placebo 20%) [7]
- May not be suitable for patients with recurrent migraines [2]
- Insomnia (14%; placebo 5%) [7]
- Includes initial, middle, and terminal insomnia; consistent with the activating profile of 5-HT1A agonism [2,3]
- Clinical tip: morning dosing may reduce insomnia; assess for caffeine intake and sleep hygiene before adding a hypnotic
- Paresthesia (4%; placebo 1%) [7]
- Agitation, jitteriness (3%; placebo 0%) [7]
- Lethargy (2%; placebo 0%) [7]
Gastrointestinal
- Nausea (35%; placebo 13%) [7]
- Second most common adverse reaction; typically emerges during titration and improves over time [2,3]
- Taking gepirone with food (required per labeling for absorption) also reduces the GI tolerability burden [7]
- Vomiting (7% incidence; placebo 4%) [7]
- Abdominal pain (7% incidence; placebo 3%) [7]
- Dyspepsia (6% incidence; placebo 2%) [7]
- Dry mouth (8% incidence; placebo 5%) [7]
- Diarrhea (10% incidence; placebo 9%) [7]
- Rates not meaningfully different from placebo
- Constipation (4% incidence; placebo 3%) [7]
- Increased appetite (5% incidence; placebo 3%) [7]
Cardiovascular
- Palpitations (4% incidence; placebo 0%) and increased heart rate (2% incidence; placebo 0%) [7]
- Mild, generally do not require dose adjustment in the absence of QTc prolongation
- Likely reflect the noradrenergic activity of the 1-PP metabolite
- In a drug that prolongs QTc, monitor for symptomatic palpitations and obtain ECG if new arrhythmia symptoms emerge
- Orthostatic symptoms
- Although orthostatic hypotension is not specifically labeled, postural dizziness is captured under the dizziness category and may overlap mechanistically given the alpha-2 adrenergic activity of the 1-PP metabolite [2,7]
Other common side effects
- Upper respiratory tract infection (8% incidence; placebo 7%), nasopharyngitis (4%; placebo 3%), nasal congestion (4%; placebo 2%) [7]
- Hyperhidrosis (4% incidence; placebo 0%) [7]
- Hypersensitivity reactions
- Rash, pruritus, and urticaria were reported in clinical studies [7]
- Discontinue if hypersensitivity is suspected
Severe or rare side effects
QT prolongation
- The most clinically significant safety concern: gepirone produces dose-dependent prolongation of the QTc interval and can precipitate torsades de pointes or other life-threatening arrhythmias [7]
- Mean QTc increase ~16–18 msec at exposures ~2× the maximum recommended therapeutic dose [7]
- Contraindicated in patients with [7]
- Baseline QTc > 450 msec
- Congenital long QT syndrome
- Concomitant use of strong CYP3A4 inhibitors (which can raise gepirone exposure ~5-fold)
- Mandatory monitoring [7]
- Baseline ECG before initiation; do not start if QTc > 450 msec
- Repeat ECG with each dose escalation, then periodically during maintenance
- Monitor more frequently with concomitant QT-prolonging drugs, in patients who develop QTc ≥ 450 msec, or in those at significant risk of torsades de pointes
- Do not escalate the dose if QTc > 450 msec at any point
- Correct hypokalemia and hypomagnesemia prior to initiation, especially in patients on diuretics or glucocorticoids [3,7]
Serotonin syndrome
- Rare with monotherapy; risk increases with serotonergic combinations [7]
- Contraindicated with MAOIs, including IV methylene blue and within 14 days of stopping an MAOI; do not start an MAOI within 14 days of discontinuing gepirone [7]
- Linezolid: per FDA labeling, concomitant use is contraindicated [7]
- Use caution and monitor with other serotonergic agents (SSRIs, SNRIs, TCAs, triptans, fentanyl, lithium, tramadol, tryptophan, St. John’s Wort, buspirone)
- See the Serotonin Syndrome Guide for recognition and management
Activation of mania or hypomania
- Class effect; screen for personal or family history of bipolar disorder before initiation [7]
Suicidal thoughts and behaviors (boxed warning)
- Per label increased risk of suicidal thinking and behavior in patients < 25 years on antidepressants generally [7]
- Monitor closely during initiation and dose changes
Discontinuation considerations
- Gepirone is not associated with the classical SSRI/SNRI discontinuation syndrome in the FDA labeling, and pivotal trials did not report a discontinuation-emergent symptom signal [2,7]
- Long-term safety data extending beyond ~1 year are limited [2]
- As with any antidepressant, gradual tapering is reasonable when feasible to assess for clinical worsening
Tolerability considerations
- Sexual function:
- Favorable profile: minimal sexual side effects, and gepirone may improve sexual desire in depressed patients [4,5,17]
- Gepirone ER was equivalent to placebo on rates of sexual side effects and treatment-emergent sexual dysfunction, and significantly lower than SSRIs in a pooled analysis of five Phase 3 RCTs (n = 1,767) [4]
- In some subgroups, gepirone produced rates of sexual dysfunction lower than placebo
- In men with MDD, gepirone improved CSFQ scores across all sexual function domains, including in antidepressant non-responders—suggesting a pro-sexual effect independent of mood improvement [5]
- Favorable profile: minimal sexual side effects, and gepirone may improve sexual desire in depressed patients [4,5,17]
- Weight:
- Weight-neutral: weight increase reported in 3% vs. 1% on placebo (not clinically significant), with no clinically significant changes in body weight across pivotal trials [2,7,18,19]
- See the Antidepressant-Induced Weight Gain Guide
Use in special populations
Pregnancy
- Limited human data; due to lack of data
- Agents other than gepirone are preferred for use during pregnancy [7]
- For treatment-naive patients in pregnancy, agents with more robust human safety data (e.g., sertraline, fluoxetine) are generally preferred [20,21]
- Animal studies showed fetal growth restriction and increased postnatal mortality at human-equivalent doses; no malformations were observed [7]
Breastfeeding
- No human lactation data; gepirone is present in rat milk [7]
- For treatment-naive breastfeeding patients, antidepressants with established lactation safety data (e.g., sertraline, paroxetine) are preferred [21,22]
Hepatic impairment
- Mild impairment (Child-Pugh A)
- No dosage adjustment necessary [2,7]
- Moderate impairment (Child-Pugh B)
- Initial dose: 18.2 mg once daily
- Maximum dose: 36.3 mg once daily (after Day 7), based on response and tolerability [2,7]
- Decreased metabolism of gepirone and its major metabolites (1-PP and 3’-OH-gepirone) has been documented [7]
- Severe impairment (Child-Pugh C)
- Contraindicated [2,7]
- Reduced hepatic clearance increases systemic exposure and may compound the dose-dependent QTc prolongation risk
Renal impairment
- Severe renal impairment is associated with approximately a 2-fold rise in gepirone Cmax and a prolonged half-life of the active metabolite 1-PP, while the parent drug’s half-life remains relatively stable [2]
- CrCl ≥ 50 mL/min
- No dosage adjustment necessary [2,7]
- CrCl < 50 mL/min
- Initial dose: 18.2 mg once daily
- Maximum dose: 36.3 mg once daily (after Day 7), based on response and tolerability [2,7]
Elderly
- Geriatric exposure (AUC and Cmax) is higher than in younger adults
- Start at 18.2 mg once daily; maximum 36.3 mg/day after 7 days [2,7]
Brand names
- US: Exxua, Exxua Titration Pack [7]
- Canada: Not currently approved
- Other countries/regions: Not currently approved as of April 2026
References
1. Turner, E. H., Powers, J. H., Ahn-Horst, R. Y., & Kesselheim, A. S. (2026). Assessing Drug Efficacy After Multiple Negative Trials—Gepirone’s Journey Through the FDA. JAMA Psychiatry. https://doi.org/10.1001/jamapsychiatry.2026.1438
2. Gałka, N., Tomaka, E., Tomaszewska, J., Pańczyszyn-Trzewik, P., & Sowa-Kućma, M. (2025). Gepirone for Major Depressive Disorder: From Pharmacokinetics to Clinical Evidence: A Narrative Review. International Journal of Molecular Sciences, 26(19), 9805. https://doi.org/10.3390/ijms26199805
3. Phillips, B., O’Connor, C., & St. Onge, E. (2024). Gepirone: A New Extended-Release Oral Selective Serotonin Receptor Agonist for Major Depressive Disorder. Journal of Pharmacy Technology, 40(5), 230–235. https://doi.org/10.1177/87551225241269179
4. Lorenz, T. K., Johnson, M. F., & Clayton, A. H. (2024). Effects of Gepirone-ER on Sexual Function in Patients With Major Depressive Disorder. The Journal of Clinical Psychiatry, 85(4), 24m15357. https://doi.org/10.4088/JCP.24m15357
5. Fabre, L. F., Clayton, A. H., Smith, L. C., Goldstein, I., & Derogatis, L. R. (2012). The effect of gepirone-ER in the treatment of sexual dysfunction in depressed men. The Journal of Sexual Medicine, 9(3), 821–829. https://doi.org/10.1111/j.1743-6109.2011.02624.x
6. Alpert, J. E., Franznick, D. A., Hollander, S. B., & Fava, M. (2004). Gepirone extended-release treatment of anxious depression: Evidence from a retrospective subgroup analysis in patients with major depressive disorder. The Journal of Clinical Psychiatry, 65(8), 1069–1075. https://www.ncbi.nlm.nih.gov/pubmed/15323591
7. Food, U. S., & Administration, D. (2023). EXXUA (gepirone) extended-release tablets. https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/021164s000lbl.pdf
8. Keam, S. J. (2023). Gepirone Extended-Release: First Approval. Drugs, 83(18), 1723–1728. https://doi.org/10.1007/s40265-023-01975-5
9. Blier, P., & Ward, N. M. (2003). Is there a role for 5-HT1A agonists in the treatment of depression? Biological Psychiatry, 53(3), 193–203. https://doi.org/10.1016/S0006-3223(02)01643-8
10. Greenblatt, D. J., Von Moltke, L. L., Giancarlo, G. M., & Garteiz, D. A. (2003). Human cytochromes mediating gepirone biotransformation at low substrate concentrations. Biopharmaceutics & Drug Disposition, 24(2), 87–94. https://doi.org/10.1002/bdd.340
11. Fabre, L. F., & Timmer, C. J. (2003). Effects of food on the bioavailability of gepirone from extended-release tablets in humans: Results of two open-label crossover studies. Current Therapeutic Research, Clinical and Experimental, 64(8), 580–598. https://doi.org/10.1016/j.curtheres.2003.09.012
12. Yang, Z., Hossain, M. A., Zhang, Q., Liu, L., Singleton, C. A., Markowitz, J. S., & Greenblatt, D. J. (2025). Ketoconazole Inhibition of Gepirone Biotransformation and Clearance: In Vitro and Clinical Studies. Journal of Clinical Pharmacology, 65(11), 1433–1442. https://doi.org/10.1002/jcph.70059
13. Bai, A. D., McKenna, S., Wise, H., Loeb, M., & Gill, S. S. (2022). Association of Linezolid With Risk of Serotonin Syndrome in Patients Receiving Antidepressants. JAMA Network Open, 5(12), e2247426. https://doi.org/10.1001/jamanetworkopen.2022.47426
14. Butterfield, J. M., Lawrence, K. R., Reisman, A., Huang, D. B., Thompson, C. A., & Lodise, T. P. (2012). Comparison of serotonin toxicity with concomitant use of either linezolid or comparators and serotonergic agents: An analysis of Phase III and IV randomized clinical trial data. The Journal of Antimicrobial Chemotherapy, 67(2), 494–502. https://doi.org/10.1093/jac/dkr467
15. Karkow, D. C., Kauer, J. F., & Ernst, E. J. (2017). Incidence of Serotonin Syndrome With Combined Use of Linezolid and Serotonin Reuptake Inhibitors Compared With Linezolid Monotherapy. Journal of Clinical Psychopharmacology, 37(5), 518–523. https://doi.org/10.1097/JCP.0000000000000751
16. Kufel, W. D., Parsels, K. A., Blaine, B. E., Steele, J. M., Seabury, R. W., & Asiago-Reddy, E. A. (2023). Real-world evaluation of linezolid-associated serotonin toxicity with and without concurrent serotonergic agents. International Journal of Antimicrobial Agents, 62(1), 106843. https://doi.org/10.1016/j.ijantimicag.2023.106843
17. Fabre, L. F., Brown, C. S., Smith, L. C., & Derogatis, L. R. (2011). Gepirone-ER treatment of hypoactive sexual desire disorder (HSDD) associated with depression in women. The Journal of Sexual Medicine, 8(5), 1411–1419. https://doi.org/10.1111/j.1743-6109.2011.02216.x
18. Feiger, A. D., Heiser, J. F., Shrivastava, R. K., Weiss, K. J., Smith, W. T., Sitsen, J. M. A., & Gibertini, M. (2003). Gepirone extended-release: New evidence for efficacy in the treatment of major depressive disorder. The Journal of Clinical Psychiatry, 64(3), 243–249. https://www.ncbi.nlm.nih.gov/pubmed/12716264
19. Bielski, R. J., Cunningham, L., Horrigan, J. P., Londborg, P. D., Smith, W. T., & Weiss, K. (2008). Gepirone extended-release in the treatment of adult outpatients with major depressive disorder: A double-blind, randomized, placebo-controlled, parallel-group study. The Journal of Clinical Psychiatry, 69(4), 571–577. https://doi.org/10.4088/jcp.v69n0408
20. Treatment and Management of Mental Health Conditions During Pregnancy and Postpartum: ACOG Clinical Practice Guideline No. 5. (2023). Obstetrics and Gynecology, 141(6), 1262–1288. https://doi.org/10.1097/AOG.0000000000005202
21. MacQueen, G. M., Frey, B. N., Ismail, Z., Jaworska, N., Steiner, M., Lieshout, R. J. V., Kennedy, S. H., Lam, R. W., Milev, R. V., Parikh, S. V., Ravindran, A. V., & CANMAT Depression Work Group. (2016). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 6. Special Populations: Youth, Women, and the Elderly. Canadian Journal of Psychiatry. Revue Canadienne De Psychiatrie, 61(9), 588–603. https://doi.org/10.1177/0706743716659276
22. Sriraman, N. K., Melvin, K., Meltzer-Brody, S., & the Academy of Breastfeeding Medicine. (2015). ABM Clinical Protocol #18: Use of Antidepressants in Breastfeeding Mothers. Breastfeeding Medicine, 10(6), 290–299. https://doi.org/10.1089/bfm.2015.29002
