
In a nutshell
Dextromethorphan/Bupropion (DXM/BUP) is the first oral NMDA receptor antagonist approved for major depressive disorder (MDD) and the first non-antipsychotic drug approved for agitation associated with dementia due to Alzheimer’s disease.
Bupropion inhibits dextromethorphan’s metabolism, increasing its bioavailability.
In MDD, its primary clinical advantage is a rapid onset of antidepressant effect.
In Alzheimer’s agitation, it offers a non-antipsychotic option that avoids the boxed mortality warning carried by atypical antipsychotics.
Potent CYP2D6 inhibition, seizure risk, hyponatremia risk in older adults, and abuse potential call for careful patient selection and monitoring across both indications.

| Major Depressive Disorder | Alzheimer’s Agitation | |
|---|---|---|
| Consider when | • Rapid antidepressant response is a priority • Inadequate response to first-line SSRI/SNRI • Depression with prominent fatigue or anhedonia (bupropion component) • SSRI/SNRI-associated sexual dysfunction is a concern | • Moderate-to-severe persistent agitation requiring pharmacological intervention • Avoidance of antipsychotic exposure is a priority • Scheduled twice-daily dosing is feasible (not for prn use) |
| Alternative | Esketamine: indicated for TRD; DXM/BUP failed to maintain superiority beyond week 2 in TRD trials [1,2] | Brexpiprazole: first approved for this indication (2023) but carries the antipsychotic-class boxed mortality warning; no head-to-head data with DXM/BUP [3] |
| Indication-specific cautions | • Pregnancy or breastfeeding | • Geriatric hyponatremia risk (esp. with diuretics or serotonergic antidepressants) • Falls risk compounded by baseline gait/cognitive impairment • Concurrent cholinesterase inhibitors (donepezil, galantamine) which are CYP2D6 substrates |
Contraindications
- Seizure disorder or history of eating disorder (anorexia/bulimia)
- Abrupt discontinuation of alcohol, benzodiazepines, barbiturates, or antiepileptics
- Concurrent or recent (within 14 days) MAOI use
- Known hypersensitivity to bupropion or dextromethorphan
Other prescribing considerations
- Active substance-use disorder or concern for dextromethorphan diversion
- High drug-interaction burden through CYP2D6 (potent inhibitor, see Pharmacokinetics)
- Cost is a significant barrier
Pharmacodynamics and mechanism of action
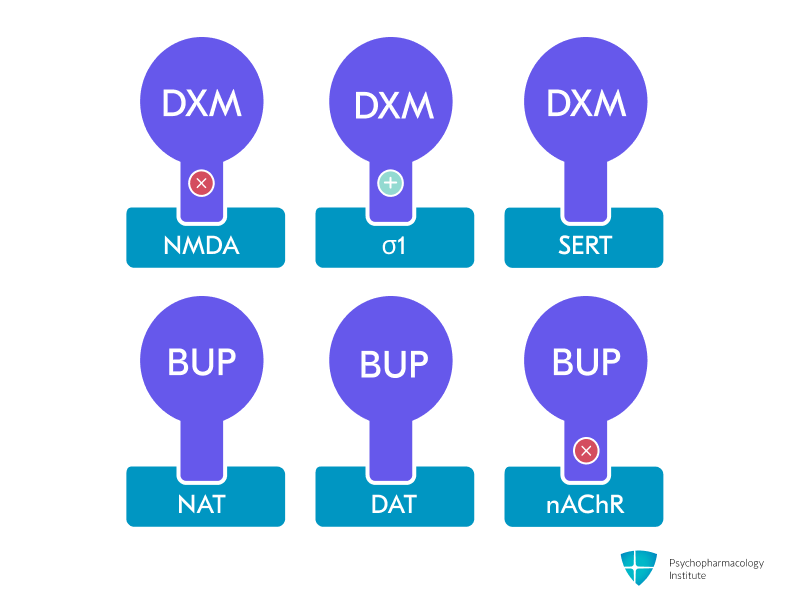
- Dextromethorphan (DXM) component:
- Uncompetitive NMDA-receptor antagonist and high-affinity σ-1 receptor agonist [3]
- Additional actions: SERT/NET inhibition, nicotinic α4β2 antagonism, weak μ-opioid agonism. [4]
- NMDA receptor antagonism (dextromethorphan)
- Provides glutamatergic modulation similar to ketamine and esketamine [4]
- NMDA blockade indirectly enhances AMPA receptor signaling, increases BDNF release, and activates mTOR, driving synaptogenesis and dendritic spine formation in the prefrontal cortex [5–7]
- In MDD: the proposed substrate for rapid antidepressant onset, with separation from placebo by week 1 in the GEMINI trial [4,8]
- In Alzheimer’s agitation: may modulate the excitotoxic glutamatergic signaling implicated in the neuropsychiatric symptoms of dementia, though the precise mechanism is not established [3]
- σ-1 receptor agonism (dextromethorphan)
- Modulates neuroplasticity and exerts neuroprotective effects [9,10]
- In MDD: may contribute to antidepressant effect through plasticity and neuroprotective pathways [5]
- In Alzheimer’s agitation: proposed but unconfirmed contributor to the anti-agitation effect [3]
- Bupropion component:
- Pharmacokinetic role:
- CYP2D6 blockade raises dextromethorphan exposure and extends its half-life ~3-fold to 22 hours, enabling clinically meaningful brain levels of DXM from an oral combination [3]
- In MDD: contributes traditional monoaminergic antidepressant activity; the combination outperformed bupropion alone in the ASCEND trial, confirming that dextromethorphan adds incremental efficacy [11]
- In Alzheimer’s agitation: bupropion’s monoaminergic effects do not appear to drive the anti-agitation response; the bupropion-only arm of the ADVANCE trial was terminated for futility [3]
- Pharmacokinetic role:
Pharmacokinetics
Metabolism and Pharmacokinetic Interactions
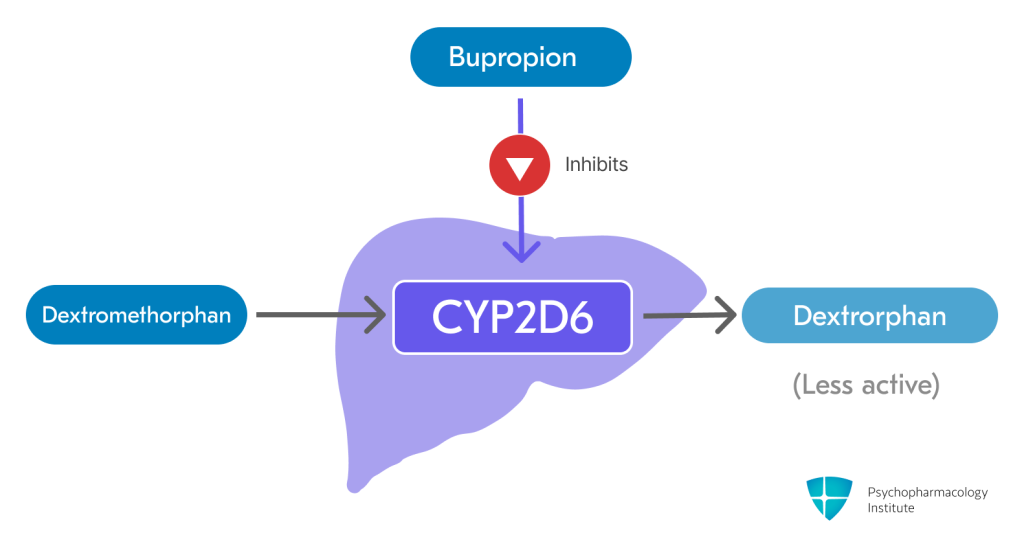
- Dextromethorphan is primarily metabolized by the CYP2D6 enzyme to its major, less active metabolite, dextrorphan [3]
- Bupropion and its metabolites are strong, competitive inhibitors of CYP2D6 [3]
- This inhibition significantly increases the plasma concentration and extends the half-life of dextromethorphan
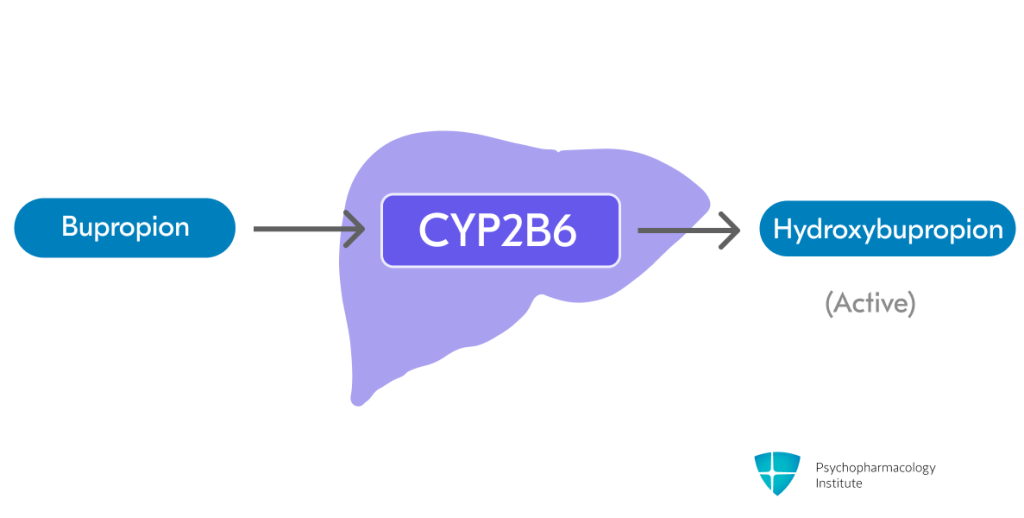
- Bupropion is metabolized in the liver through CYP2B6 to form active metabolite hydroxybupropion (primary pathway) [3,12]
- Threohydrobupropion and erythrohydrobupropion are formed through non-CYP-mediated metabolism (secondary pathway)
- Dextromethorphan/Bupropion levels increased by:
- Strong CYP2D6 inhibitors (e.g., paroxetine, fluoxetine, quinidine)
- Further increase dextromethorphan concentrations beyond the effect of bupropion alone
- Reduce Dextromethorphan/Bupropion dose to one tablet once daily in the morning [3]
- CYP2B6 Inhibitors (e.g., clopidogrel)
- May increase plasma concentrations of both bupropion and dextromethorphan.
- Monitor for adverse effects [3]
- Strong CYP2D6 inhibitors (e.g., paroxetine, fluoxetine, quinidine)
- Dextromethorphan/Bupropion levels decreased by:
- Strong CYP2B6 inducers (e.g., carbamazepine, rifampin, phenytoin, efavirenz)
- Significantly decrease plasma concentrations of both bupropion and dextromethorphan, which may reduce efficacy
- Co-administration should be avoided [3]
- Strong CYP2B6 inducers (e.g., carbamazepine, rifampin, phenytoin, efavirenz)
- Bupropion and its metabolites may increase levels of CYP2D6 substrates, including:
- Antidepressants (venlafaxine, duloxetine, nortriptyline, imipramine, desipramine, paroxetine, fluoxetine, sertraline)
- Vortioxetine dose should be reduced by 50% when used with bupropion. Consider alternative options.
- Antipsychotics (haloperidol, risperidone, aripiprazole)
- Combined use with iloperidone lowers seizure threshold and augments QT-prolongation risk. Consider alternative options.
- Beta-blockers (metoprolol)
- Type 1C antiarrhythmics (propafenone, flecainide)
- Cholinesterase inhibitors used in Alzheimer’s disease (donepezil, galantamine)
- Monitor for cholinergic adverse effects (bradycardia, GI upset, syncope) when co-administered with Dextromethorphan/Bupropion
- Consider dose reduction of CYP2D6 substrates when used concomitantly
- Conversely, drugs that require CYP2D6 for activation (e.g., tamoxifen) may have reduced efficacy
- Antidepressants (venlafaxine, duloxetine, nortriptyline, imipramine, desipramine, paroxetine, fluoxetine, sertraline)
Pharmacodynamic Interactions
- MAOIs
- Contraindicated due to high risk of hypertensive crisis and serotonin syndrome
- A 14-day washout period is required when switching to or from an MAOI [3]
- Serotonergic drugs (e.g., SSRIs, SNRIs, TCAs, triptans)
- Concomitant use increases the risk of serotonin syndrome
- Monitor closely for symptoms. If serotonin syndrome occurs, discontinue [3]
- Concomitant serotonergic antidepressants also increase the risk of hyponatremia [3]
- This is a particular concern in elderly patients with Alzheimer’s agitation
- Drugs that lower seizure threshold (e.g., other antidepressants, antipsychotics, theophylline, systemic corticosteroids)
- Additive risk of seizures due to the bupropion component
- Use with extreme caution. If a seizure occurs, Dextromethorphan/Bupropion must be permanently discontinued [3]
- Dopaminergic drugs (e.g., levodopa, amantadine)
- May increase the risk of CNS toxicity (restlessness, agitation, tremor)
- Use with caution and monitor for adverse effects [3]
- Digoxin
- Bupropion may decrease plasma digoxin levels.
- Monitor digoxin levels upon initiation of co-administration [3]
- Alcohol
- May increase the risk of neuropsychiatric adverse events or reduce alcohol tolerance
- Alcohol consumption should be minimized or avoided [3]
- False-positive drug screens
- Bupropion can cause false-positive urine immunoassay tests for amphetamines [13,14]
- Confirmatory tests (e.g., GC/MS) will distinguish bupropion from amphetamines
Half-life
- After reaching steady state (within 8 days), the mean elimination half-life is:
- Dextromethorphan: ~22 hours [3]
- Bupropion: ~15 hours [3]
- Bupropion’s active metabolites have longer half-lives (threohydrobupropion: ~33 hours; erythrohydrobupropion: ~44 hours)
Dosage forms
- Extended-release:
- Tablets
- 45 mg dextromethorphan hydrobromide / 105 mg bupropion hydrochloride
- Used for MDD and as the target/maintenance strength in Alzheimer’s agitation
- 30 mg dextromethorphan hydrobromide / 105 mg bupropion hydrochloride
- New strength introduced for the Alzheimer’s agitation titration; not used in MDD [3]
- Auvelity
- 45 mg dextromethorphan hydrobromide / 105 mg bupropion hydrochloride
- Tablets
- Generic substitution considerations:
- Dextromethorphan:
- Available as prescription or over-the-counter generic syrup (7.5 mL typically equals 45 mg dose)
- Significantly lower cost (~$20/month vs $1,200/month for branded combination)
- Bupropion:
- Generic immediate-release: 100 mg twice daily or 200 mg once daily provides similar dosing to the 105 mg component in branded combination
- Dextromethorphan:
- Formulation considerations:
- May be taken with or without meals
- Tablets must be swallowed whole
- Cannot be crushed, divided, or chewed
Indications
FDA-Approved Indications
Major Depressive Disorder (MDD)
- First oral NMDA receptor antagonist combination approved for adults with MDD [3]
- Rapid onset of action
- Separation from placebo on MADRS by week 1 and sustained superiority at week 6 in the pivotal GEMINI trial [3,8]
- Superior to bupropion SR alone
- The ASCEND study reported separation from bupropion SR at week 6, supporting the specific contribution of dextromethorphan to overall efficacy [11]
- May be considered for patients requiring faster symptom relief or those with inadequate response to first-line antidepressants
- However, limited long-term comparative data, high cost, and dextromethorphan’s diversion potential can temper routine use [1]
- Durability question: an unpublished TRD trial showed early separation from bupropion at weeks 1–2, but this advantage was not maintained at week 6, highlighting the need for confirmatory results [1,2]
- Dosing:
- Starting dose: one tablet (45 mg dextromethorphan / 105 mg bupropion) once daily in the morning [3]
- Target dose: after 3 days, increase to the maximum recommended dosage of one tablet twice daily, with doses separated by at least 8 hours [3]
- Maximum dose: 90 mg dextromethorphan / 210 mg bupropion (two tablets per day) [3]
- Strong CYP2D6 inhibitors or known CYP2D6 poor metabolizers: one 45/105 mg tablet once daily [3]
Agitation Associated with Dementia Due to Alzheimer’s Disease
- First non-antipsychotic medication FDA-approved for this indication (April 2026), and the second drug overall after brexpiprazole [3,15]
- Clinical positioning
- Offers an option for patients with moderate-to-severe agitation requiring pharmacological intervention, particularly when avoiding the antipsychotic-class boxed mortality warning is a priority
- Non-pharmacological strategies remain first-line and should continue alongside pharmacological treatment
- Not indicated for as-needed (“prn”) treatment of acute agitation episodes
- Efficacy was established only with scheduled twice-daily dosing [3]
- Evidence base
- Acute efficacy (ADVANCE, N=366, NCT03226522):
- Significant reduction in agitation in a 5-week, double-blind, placebo-controlled RCT in patients aged 65–90 with probable Alzheimer’s disease and moderate-to-severe agitation
- The bupropion-only comparator arm was halted for futility [3]
- Maintenance (ACCORD-2, N=456, NCT04947553):
- Responders continued on DXM/BUP had a statistically significantly longer time to relapse than those switched to placebo in a long-term randomized-withdrawal study
- 26-week relapse rate of ≈10% on active drug vs. ≈30% on placebo [3]
- Acute efficacy (ADVANCE, N=366, NCT03226522):
- Dosing (titration schedule differs from MDD)
- Day 1–7: one 30 mg / 105 mg tablet once daily in the morning [3]
- Day 8: increase to 30 mg / 105 mg twice daily (≥8 hours apart), based on tolerability
- Day 15: increase to the maximum recommended dose of 45 mg / 105 mg twice daily (≥8 hours apart), based on tolerability
- Do not exceed two doses within the same day [3]
- Strong CYP2D6 inhibitors, known CYP2D6 poor metabolizers, or moderate renal impairment: do not advance beyond 45/105 mg once daily (see Use in Special Populations) [3]
- Monitoring before initiation
- Assess blood pressure at baseline and periodically (bupropion component)
- Baseline sodium with recheck during the first weeks of treatment in elderly patients on diuretics or concurrent serotonergic antidepressants [3]
- Fall-risk assessment: dizziness, somnolence, and gait-related events are common in this population [3]
Off-label Uses
- Treatment-resistant depression and cognitive/anxiety symptoms in MDD are being explored in open-label and extension studies (e.g., COMET-TRD, EVOLVE); evidence is preliminary and not guideline-endorsed [1]
- There are currently no other well-established off-label uses for the dextromethorphan-bupropion combination.
Side effects
Most common side effects
The adverse-reaction profile differs by indication. Incidences below are from the pivotal placebo-controlled trials.
| Adverse event | MDD¹ | Alzheimer’s agitation² |
|---|---|---|
| Neurological | ||
| Dizziness | 16% | 9% |
| Somnolence | 7% | 8% |
| Headache | 8% | 4% |
| Fatigue | — | 6% |
| Confusional state | — | 3% |
| Gastrointestinal | ||
| Nausea | 13% | 5% |
| Diarrhea | 7% | — |
| Dyspepsia | — | 6% |
| Dry mouth | 6% | 4% |
| Constipation | 4% | 3% |
| Psychiatric / other | ||
| Sexual dysfunction | 6% | — |
| Hyperhidrosis | 5% | — |
| Anxiety | 4% | — |
| Insomnia | 4% | — |
| Psychotic symptoms | — | 3% |
| Cough | — | 3% |
| Bacterial infection | — | 3% |
¹ GEMINI, 6-week placebo-controlled MDD trial (N=162); discontinuation due to AEs 4% (vs. 0% placebo) [3,8]
² ADVANCE, 5-week placebo-controlled AD-agitation trial (N=159); discontinuation due to AEs 1.3% (vs. 1.3% placebo) [3]
Clinical management
- Cross-indication
- Dizziness
- Most common side effect [3,8]
- Take precautions to reduce fall risk, particularly in patients with motor impairment or a history of falls
- Caution patients about operating machinery and driving until they know how dextromethorphan/bupropion affects them
- Somnolence
- Despite containing bupropion, which is typically activating
- Consider morning dosing if sedation persists
- Nausea
- Can be minimized by taking with food and usually improves within the first week
- In MDD it is less likely to lead to discontinuation than with SSRIs [8]
- Anxiety
- Leading reason for discontinuation (2% of patients in in GEMINI trial)
- Monitor during initial titration [3]
- Insomnia
- Keep doses ≥8 hours apart and avoid evening dosing
- Hyperhidrosis may require dose adjustment if bothersome
- Dizziness
- MDD-specific
- Sexual dysfunction
- Significantly lower than SSRIs/SNRIs
- Bupropion component may actually mitigate sexual side effects [16]
- Consider Dextromethorphan/Bupropion for patients with SSRI-induced sexual dysfunction
- Sexual dysfunction
- Alzheimer’s-agitation-specific
- Psychotic symptoms (3% on active drug vs. 0% placebo)
- Pooled term including catatonia, delusion, and hallucinations (visual or otherwise)
- Counsel caregivers to report new perceptual disturbances [3]
- Confusional state (3%)
- Includes delirium and disorientation [3]
- Can be difficult to distinguish from baseline dementia progression and may warrant a treatment hold
- Fall risk is compounded by baseline gait and cognitive impairment
- Psychotic symptoms (3% on active drug vs. 0% placebo)
Severe side effects
- Seizures
- Dose-related risk inherent to bupropion [3]
- Contraindicated in patients with seizure disorder, eating disorders (especially bulimia), or undergoing abrupt discontinuation of alcohol/benzodiazepines
- Risk factors include: head trauma, CNS tumors, metabolic disorders, concomitant medications lowering seizure threshold [3]
- Do not exceed the maximum dose of 2 tablets daily. Screen patients for use of other bupropion-containing products before initiating treatment.
- Hypertension and cardiovascular effects
- Risk increased with MAOIs, nicotine replacement, or drugs that increase dopaminergic/noradrenergic activity [3]
- Monitor blood pressure before initiation and periodically during treatment
- Use caution in patients with pre-existing hypertension or cardiovascular disease
- Hyponatremia (updated in 2026 label)
- Can occur with Dextromethorphan/Bupropion, often via SIADH
- One case with serum sodium 115 mmol/L was reported in premarketing studies [3]
- Geriatric patients are at greater risk, which is relevant to the Alzheimer’s agitation population
- Risk is increased by concomitant serotonergic antidepressants, diuretics, or volume depletion
- Symptoms (headache, difficulty concentrating, memory impairment, confusion, weakness, unsteadiness leading to falls) overlap substantially with dementia progression [3]
- Maintain a low threshold to check a sodium level if a patient appears clinically worse
- Can occur with Dextromethorphan/Bupropion, often via SIADH
- Activation of mania/hypomania
- As with other antidepressants, there is a risk of precipitating a manic or hypomanic episode. Screen for bipolar disorder before initiation [3]
- Case report described dextromethorphan-induced manic symptoms in a bipolar patient on lithium [17]
- The combination of dextromethorphan and memantine was assessed in a clinical trial for treating bipolar disorder [18]
- Monitor for the emergence of manic symptoms, especially in the first few weeks
- Serotonin syndrome
- Risk with concomitant SSRIs, SNRIs, tricyclics, triptans, or other serotonergic agents [3]
- Contraindicated with MAOIs (14-day washout required) [3]
- Monitor for symptoms: hyperthermia, muscle rigidity, autonomic instability, mental status changes
- Psychosis and neuropsychiatric reactions
- Bupropion can cause delusions, hallucinations, paranoia, confusion [3,19]
- Dextromethorphan overdose can cause toxic psychosis [20]
- Risk increased with higher doses or in predisposed individuals
- Discontinue if psychotic symptoms emerge
- 3% of patients on active drug developed psychotic symptoms (vs. 0% placebo) and 3% experienced confusion or delirium (vs. 1% placebo) in the ADVANCE trial [3]
- Counsel caregivers to report new perceptual or cognitive changes
- Angle-closure glaucoma
- Pupilary dilation induced by bupropion may trigger angle-closure attack in patients with anatomically narrow angles [3,21]
- Screen patients with narrow angles who have not had iridectomy
- Educate about symptoms: eye pain, vision changes, eye redness/swelling
Abuse potential
- Dextromethorphan is available as an over-the-counter antitussive that produces intoxicating, hallucinogenic, and dissociative effects at supra-therapeutic doses [22]
- Recreational use of DXM is sometimes referred to in slang form as “robo-tripping” or “skittling”, whose prefix derives from the Robitussin brand name, or “Triple Cs” [23]
- Fatal overdoses have been reported in cases where death was attributed to dextromethorphan toxicity [24]
- Known as “poor man’s cocaine” due to its stimulant-like effects, bupropion has earned this street name and is the most commonly misused antidepressant, with 75% increase in abuse between 2000-2012 [25–27]
- Monitor for signs of misuse, especially in patients with a substance use history
Use in special populations
Pregnancy
- Not recommended: Animal studies show fetal harm and neurotoxicity concerns.
- Manufacturer recommends discontinuing treatment in pregnant females [3]
- Use alternative treatment for women who are planning to become pregnant.
Breastfeeding
- Breast-feeding is not recommended during therapy and for 5 days after the final dose because of potential neurotoxicity [3]
- Bupropion and active metabolites appear in human milk (≈ 2% of the weight-adjusted maternal dose).
- Dextromethorphan levels in human milk are unknown.
Hepatic Impairment
- Mild to moderate impairment (Child-Pugh A or B):
- No dose adjustment needed [3]
- Severe hepatic impairment (Child-Pugh C):
- Use is not recommended (has not been studied) [3]
Renal Impairment
- Mild impairment (eGFR ≥60 mL/minute/1.73 m²):
- No dosage adjustment necessary
- Moderate impairment (eGFR 30–59 mL/minute/1.73 m²):
- MDD:
- Maximum dose is one 45/105 mg tablet once daily in the morning [3]
- Alzheimer’s agitation:
- Start 30/105 mg once daily
- On day 8 increase to 45/105 mg once daily based on tolerability
- Do not advance to twice-daily dosing [3]
- MDD:
- Severe impairment / End-stage renal disease (eGFR <30 mL/minute/1.73 m²):
- Use is not recommended (has not been studied) [3]
CYP2D6 Poor Metabolizers
- Poor metabolizers have approximately 3-fold higher dextromethorphan concentrations
- MDD:
- One 45/105 mg tablet once daily in the morning [3]
- Alzheimer’s agitation:
- Start 30/105 mg once daily
- On day 8 increase to 45/105 mg once daily based on tolerability
- Do not advance to twice-daily dosing [3]
Elderly
- MDD pivotal trials excluded patients ≥65; pharmacokinetics in geriatric volunteers were similar to younger adults [3]
- AD-agitation trials enrolled 720 patients ≥65 (including 352 ≥75); no overall differences in safety or efficacy were observed [3]
- Hyponatremia is more common in this population (see Severe side effects → Hyponatremia) [3]
- Check baseline sodium and recheck during the first weeks of treatment in patients on diuretics, with reduced oral intake, or on concurrent serotonergic antidepressants
Brand names
- US: Auvelity
References
1. McCarthy, B., Bunn, H., Santalucia, M., Wilmouth, C., Muzyk, A., & Smith, C. M. (2023). Dextromethorphan-bupropion (Auvelity) for the Treatment of Major Depressive Disorder. Clinical Psychopharmacology and Neuroscience, 21(4), 609–616. https://doi.org/10.9758/cpn.23.1081
2. Axsome Therapeutics Announces Topline Results of the STRIDE-1 Phase 3 Trial in Treatment Resistant Depression and Expert Call to Discuss Clinical Implications. BioSpace. https://www.biospace.com/axsome-therapeutics-announces-topline-results-of-the-stride-1-phase-3-trial-in-treatment-resistant-depression-and-expert-call-to-discuss-clinical-implications
3. U.S. Food and Drug Administration (2026). AUVELITY® (dextromethorphan hydrobromide and bupropion hydrochloride) extended-release tablets, for oral use. https://www.accessdata.fda.gov/drugsatfda_docs/label/2026/215430s009s018lbl.pdf
4. Stahl, S. M. (2019). Dextromethorphan/Bupropion: A Novel Oral NMDA (N-methyl-d-aspartate) Receptor Antagonist with Multimodal Activity. CNS Spectrums, 24(5), 461–466. https://doi.org/10.1017/S1092852919001470
5. Zanos, P., Moaddel, R., Morris, P. J., Riggs, L. M., Highland, J. N., Georgiou, P., Pereira, E. F. R., Albuquerque, E. X., Thomas, C. J., Zarate, C. A., & Gould, T. D. (2018). Ketamine and Ketamine Metabolite Pharmacology: Insights into Therapeutic Mechanisms. Pharmacological Reviews, 70(3), 621–660. https://doi.org/10.1124/pr.117.015198
6. McIntyre, R. S., Rosenblat, J. D., Nemeroff, C. B., Sanacora, G., Murrough, J. W., Berk, M., Brietzke, E., Dodd, S., Gorwood, P., Ho, R., Iosifescu, D. V., Lopez Jaramillo, C., Kasper, S., Kratiuk, K., Lee, J. G., Lee, Y., Lui, L. M. W., Mansur, R. B., Papakostas, G. I., … Stahl, S. (2021). Synthesizing the Evidence for Ketamine and Esketamine in Treatment-Resistant Depression: An International Expert Opinion on the Available Evidence and Implementation. American Journal of Psychiatry, 178(5), 383–399. https://doi.org/10.1176/appi.ajp.2020.20081251
7. Duman, R. S., Aghajanian, G. K., Sanacora, G., & Krystal, J. H. (2016). Synaptic plasticity and depression: New insights from stress and rapid-acting antidepressants. Nature Medicine, 22(3), 238–249. https://doi.org/10.1038/nm.4050
8. Iosifescu, D. V., Jones, A., O’Gorman, C., Streicher, C., Feliz, S., Fava, M., & Tabuteau, H. (2022). Efficacy and Safety of AXS-05 (Dextromethorphan-Bupropion) in Patients With Major Depressive Disorder: A Phase 3 Randomized Clinical Trial (GEMINI). The Journal of Clinical Psychiatry, 83(4), 21m14345. https://doi.org/10.4088/JCP.21m14345
9. Hashimoto, K. (2009). Sigma-1 receptors and selective serotonin reuptake inhibitors: Clinical implications of their relationship. Central Nervous System Agents in Medicinal Chemistry, 9(3), 197–204. https://doi.org/10.2174/1871524910909030197
10. Fishback, J. A., Robson, M. J., Xu, Y.-T., & Matsumoto, R. R. (2010). Sigma receptors: Potential targets for a new class of antidepressant drug. Pharmacology & Therapeutics, 127(3), 271–282. https://doi.org/10.1016/j.pharmthera.2010.04.003
11. Tabuteau, H., Jones, A., Anderson, A., Jacobson, M., & Iosifescu, D. V. (2022). Effect of AXS-05 (Dextromethorphan-Bupropion) in Major Depressive Disorder: A Randomized Double-Blind Controlled Trial. The American Journal of Psychiatry, 179(7), 490–499. https://doi.org/10.1176/appi.ajp.21080800
12. Costa, R., Oliveira, N. G., & Dinis-Oliveira, R. J. (2019). Pharmacokinetic and pharmacodynamic of bupropion: Integrative overview of relevant clinical and forensic aspects. Drug Metabolism Reviews, 51(3), 293–313. https://doi.org/10.1080/03602532.2019.1620763
13. Casey, E. R., Scott, M. G., Tang, S., & Mullins, M. E. (2011). Frequency of False Positive Amphetamine Screens due to Bupropion Using the Syva Emit II Immunoassay. Journal of Medical Toxicology, 7(2), 105–108. https://doi.org/10.1007/s13181-010-0131-5
14. Battini, V., Cirnigliaro, G., Giacovelli, L., Boscacci, M., Manzo, S. M., Mosini, G., Guarnieri, G., Gringeri, M., Benatti, B., Clementi, E., Dell’Osso, B., & Carnovale, C. (2023). Psychiatric and non-psychiatric drugs causing false-positive amphetamines urine test in psychiatric patients: A pharmacovigilance analysis using FAERS. Expert Review of Clinical Pharmacology. https://www.tandfonline.com/doi/abs/10.1080/17512433.2023.2211261
15. U.S. Food and Drug Administration Press Release (Thu, 04/30/2026 – 14:52). FDA Approves First Non-Antipsychotic Drug to Treat Agitation Associated with Dementia. FDA; FDA. https://www.fda.gov/news-events/press-announcements/fda-approves-first-non-antipsychotic-drug-treat-agitation-associated-dementia
16. Clayton, A. H., Warnock, J. K., Kornstein, S. G., Pinkerton, R., Sheldon-Keller, A., & McGarvey, E. L. (2004). A placebo-controlled trial of bupropion SR as an antidote for selective serotonin reuptake inhibitor-induced sexual dysfunction. The Journal of Clinical Psychiatry, 65(1), 62–67. https://doi.org/10.4088/jcp.v65n0110
17. Bostwick, J. M. (1996). Dextromethorphan-induced manic symptoms in a bipolar patient on lithium. Psychosomatics, 37(6), 571–573. https://doi.org/10.1016/S0033-3182(96)71523-2
18. Lee, S.-Y., Wang, T.-Y., Chen, S.-L., Chang, Y.-H., Chen, P.-S., Huang, S.-Y., Tzeng, N.-S., Wang, L.-J., Lee, I.-H., Chen, K.-C., Yang, Y.-K., Hong, J.-S., & Lu, R.-B. (2020). Combination of dextromethorphan and memantine in treating bipolar spectrum disorder: A 12-week double-blind randomized clinical trial. International Journal of Bipolar Disorders, 8, 11. https://doi.org/10.1186/s40345-019-0174-8
19. Omri, M., Ferhi, M., Rauschenbach, C., Ibrahim, A., Oliveira Galvao, M., & Hamm, O. (2024). Understanding De Novo Bupropion-Induced Psychosis and Its Management Strategies: A Case Report and Literature Review. Cureus. https://doi.org/10.7759/cureus.73980
20. Price, L. H., & Lebel, J. (2000). Dextromethorphan-Induced Psychosis. American Journal of Psychiatry, 157(2), 304–304. https://doi.org/10.1176/appi.ajp.157.2.304
21. Narayanan, V. (2019). Ocular Adverse Effects of Antidepressants – Need for an Ophthalmic Screening and Follow up Protocol. Ophthalmology Research: An International Journal, 1–6. https://doi.org/10.9734/or/2019/v10i330107
22. Gupta, L., Tomar, N., & Sarin, R. K. (2024). Dextromethorphan: A double-edged drug – Unveiling the pernicious repercussions of Abuse and forensic implications. Emerging Trends in Drugs, Addictions, and Health, 4, 100161. https://doi.org/10.1016/j.etdah.2024.100161
23. Stanciu, C. N., Penders, T. M., & Rouse, E. M. (2016). Recreational use of dextromethorphan, “Robotripping”-A brief review. The American Journal on Addictions, 25(5), 374–377. https://doi.org/10.1111/ajad.12389
24. Logan, B. K., Goldfogel, G., Hamilton, R., & Kuhlman, J. (2009). Five deaths resulting from abuse of dextromethorphan sold over the internet. Journal of Analytical Toxicology, 33(2), 99–103. https://doi.org/10.1093/jat/33.2.99
25. Evans, E. A., & Sullivan, M. A. (2014). Abuse and misuse of antidepressants. Substance Abuse and Rehabilitation, 5, 107–120. https://doi.org/10.2147/SAR.S37917
26. Stassinos, G. L., & Klein-Schwartz, W. (2016). Bupropion “abuse” reported to us poison centers. Journal of Addiction Medicine, 10(5), 357–362. https://doi.org/10.1097/ADM.0000000000000249
27. Kaur, J., Modesto-Lowe, V., & León-Barriera, R. (2024). Do not overlook bupropion misuse. Primary Care Companion for CNS Disorders, 26(2), 54349. https://doi.org/10.4088/PCC.23lr03685
