
Slides and Transcript
Slide 1 of 25
Let's move on to the next section, Pharmacology in Alcohol Use Disorder: Naltrexone, acamprosate and disulfiram.
Slide 2 of 25
So like I mentioned, these medications are often underutilized. I think there are a couple of reasons for that. The first is that we know from epidemiologic studies that the majority of patients with substance use disorders don't get any type of formal treatment. This is just the reality that access to addiction treatment remains limited in many places and so there's not as many chances for patients to be considered for medications. Second is that even among those who do treat alcohol use disorders, clinicians actually don't often utilize them. And then the final thing is that, compared to buprenorphine or methadone which is used for opioid use disorders, medications for alcohol are not as impactful and so there's a perception that they're not as helpful.
References:
- Saitz, R. (2014). Medications for alcohol use disorders. JAMA, 312(13), 1349.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 25
But whatever the reason, these medications I'm going to be talking about are effective, do help patients, maintain their sobriety or reduce their heavy drinking. And so as much as possible, I think we should be utilizing them.
References:
- Saitz, R. (2014). Medications for alcohol use disorders. JAMA, 312(13), 1349.

Slide 4 of 25
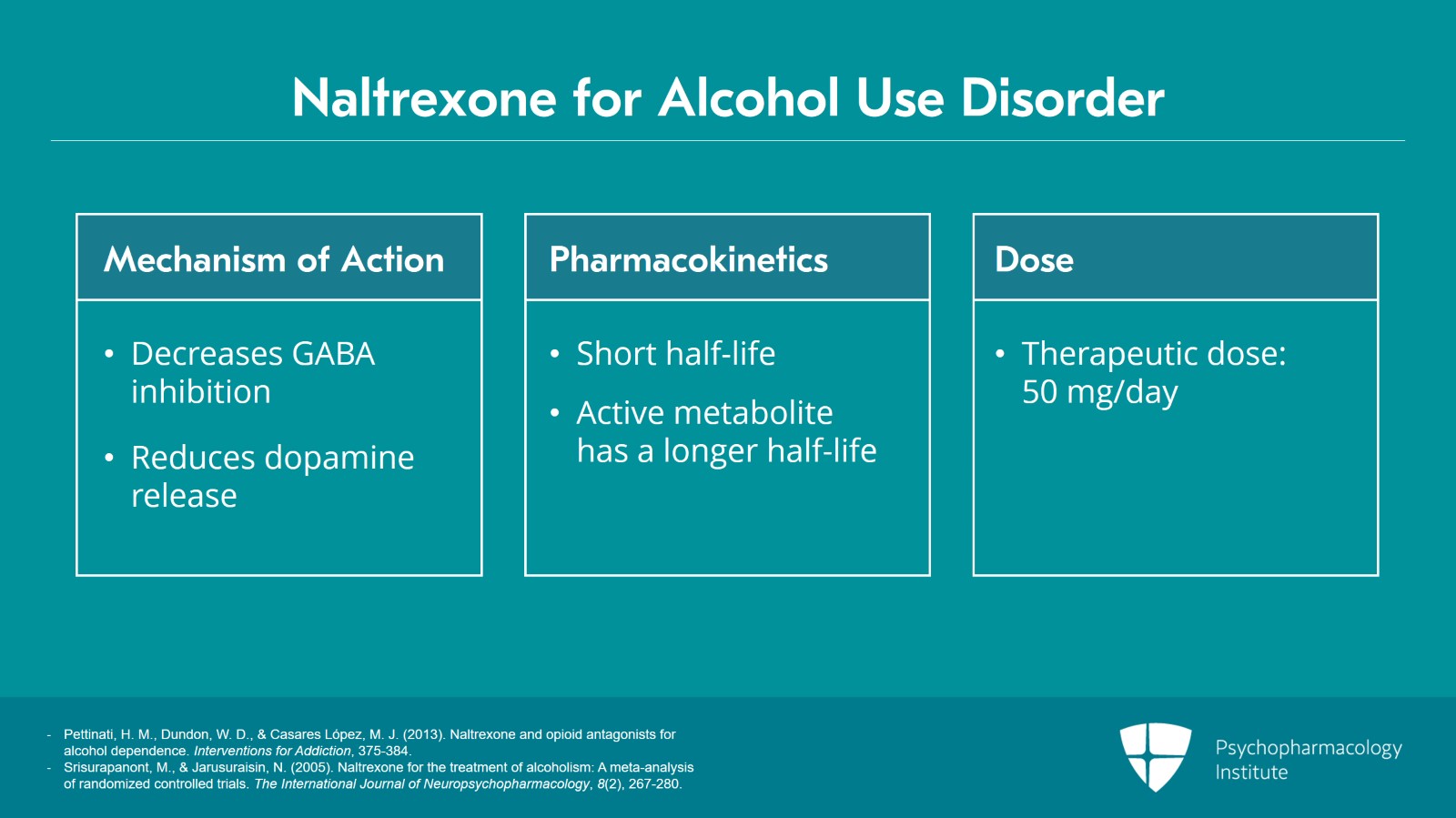
So naltrexone is the first one I'll talk about. It's a semi-synthetic mu-opioid antagonist. In terms of its mechanism of action, it's considered to decrease inhibition of GABA neurons that act to inhibit dopamine release in the mesolimbic reward pathway but net effect is that it reduces dopamine release. It has a pretty short half-life, metabolized by the liver. It has an active metabolite, 6-beta naltrexol which has a longer half-life. The therapeutic dose is really 50 mg. Sometimes, you can start with 25 and go up to 50. Many of the studies actually utilize a higher dose of 100 mg. But in clinical settings, really 50 mg a day of naltrexone is considered appropriate to start and that's it. That's your target dose.
References:
- Pettinati, H. M., Dundon, W. D., & Casares López, M. J. (2013). Naltrexone and opioid antagonists for alcohol dependence. Interventions for Addiction, 375-384.
- Srisurapanont, M., & Jarusuraisin, N. (2005). Naltrexone for the treatment of alcoholism: A meta-analysis of randomized controlled trials. The International Journal of Neuropsychopharmacology, 8(2), 267-280.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 25
The real main side effects that we're worried about are somnolence and some GI distress that can occur but it's overall well tolerated. Now, the p.o. version of naltrexone because it's metabolized in the liver can cause liver enzyme elevations and rarely hepatotoxicity and liver failure. Doing a baseline liver panel and monitoring that on some frequency is very important.
References:
- Pettinati, H. M., Dundon, W. D., & Casares López, M. J. (2013). Naltrexone and opioid antagonists for alcohol dependence. Interventions for Addiction, 375-384.
- Srisurapanont, M., & Jarusuraisin, N. (2005). Naltrexone for the treatment of alcoholism: A meta-analysis of randomized controlled trials. The International Journal of Neuropsychopharmacology, 8(2), 267-280.
Slide 6 of 25
But the current thinking is pretty clear. The damage to the liver from the drinking itself, far outweighs the risk of liver toxicity from the treatment itself. And therefore, you know, if there's mild liver enzyme elevations at baseline, it's likely because of the drinking and this should normalize under naltrexone.
References:
- Pettinati, H. M., Dundon, W. D., & Casares López, M. J. (2013). Naltrexone and opioid antagonists for alcohol dependence. Interventions for Addiction, 375-384.
- Srisurapanont, M., & Jarusuraisin, N. (2005). Naltrexone for the treatment of alcoholism: A meta-analysis of randomized controlled trials. The International Journal of Neuropsychopharmacology, 8(2), 267-280.

Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 25
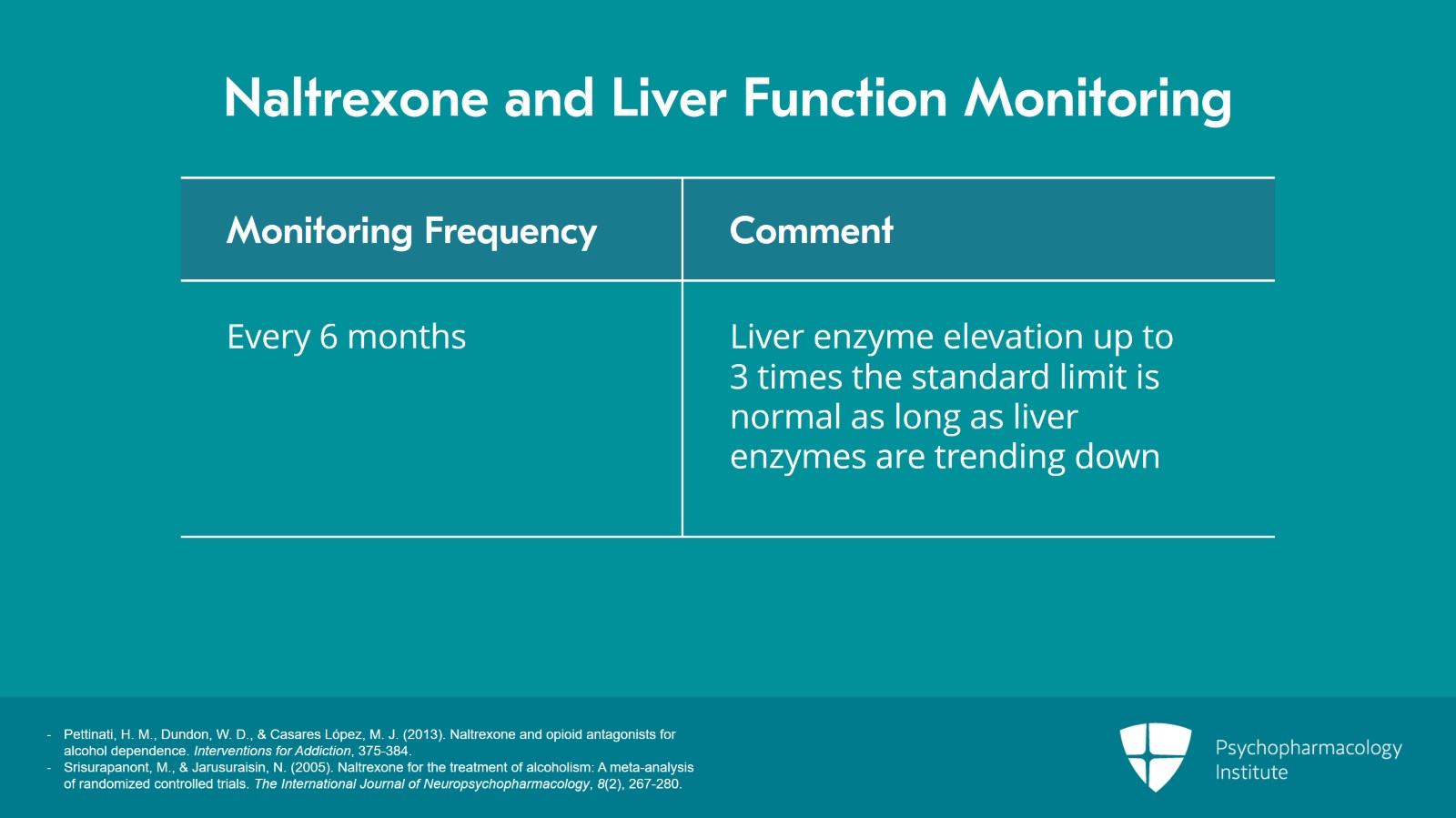
So like I mentioned, baseline LFTs are recommended and then monitoring at regular intervals like every six months. Liver enzyme elevation up to three times of normal limit will be considered okay as long as they're trending down because again the risk of liver damage from naltrexone is much less than the risk of liver damage from ongoing alcohol use. And so if the medication is providing benefit and as long as liver markers are trending down, I would still utilize this medication.
References:
- Pettinati, H. M., Dundon, W. D., & Casares López, M. J. (2013). Naltrexone and opioid antagonists for alcohol dependence. Interventions for Addiction, 375-384.
- Srisurapanont, M., & Jarusuraisin, N. (2005). Naltrexone for the treatment of alcoholism: A meta-analysis of randomized controlled trials. The International Journal of Neuropsychopharmacology, 8(2), 267-280.
Slide 8 of 25
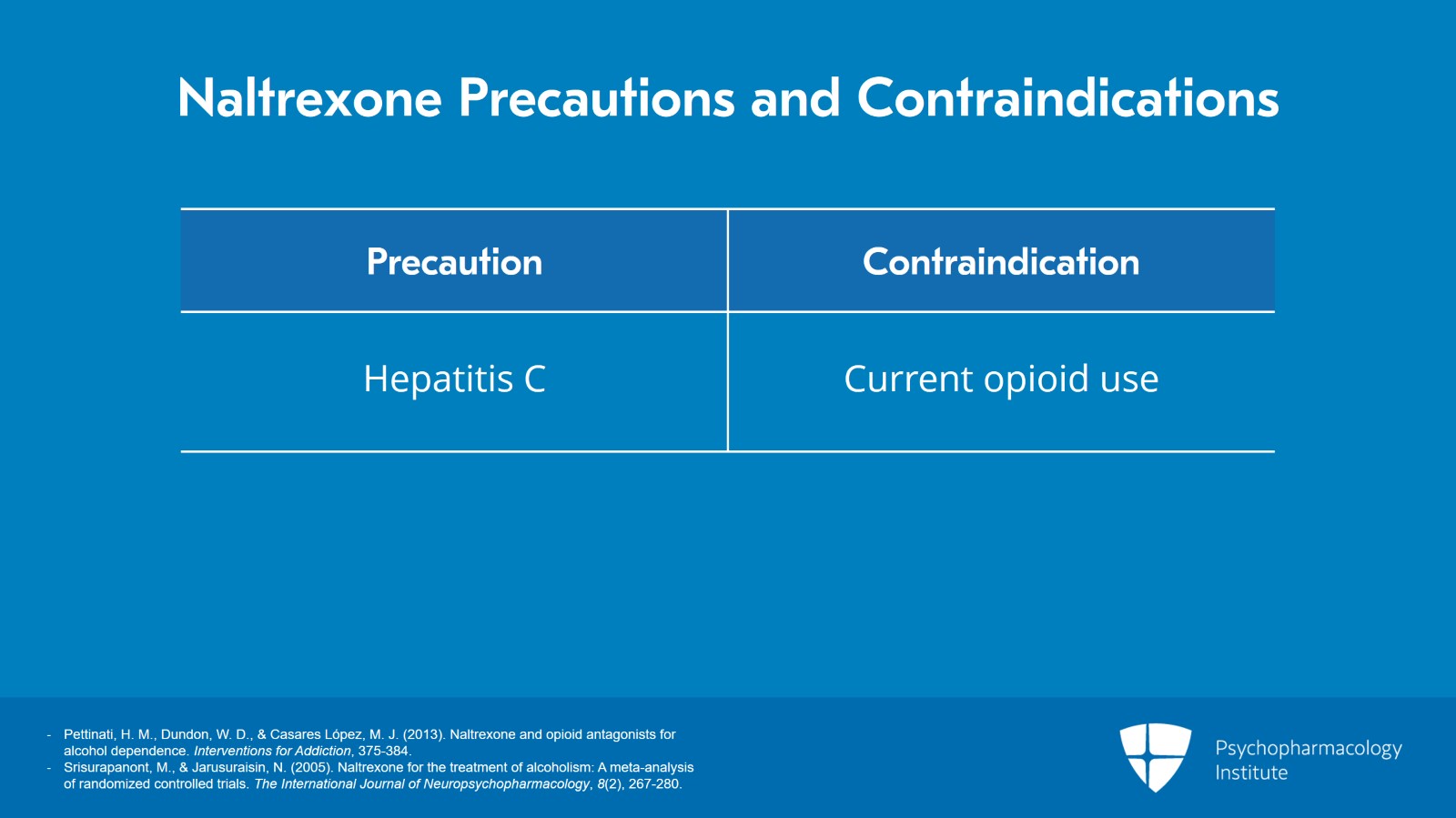
Hepatitis C is not an absolute contraindication. It warrants close monitoring. Another contraindication for naltrexone is that it's an opioid antagonist. Therefore, if the patient needs to be on opioids for whatever reason whether that's acute pain treatment, chronic pain treatment or things like buprenorphine or methadone, then it's contraindicated.
References:
- Pettinati, H. M., Dundon, W. D., & Casares López, M. J. (2013). Naltrexone and opioid antagonists for alcohol dependence. Interventions for Addiction, 375-384.
- Srisurapanont, M., & Jarusuraisin, N. (2005). Naltrexone for the treatment of alcoholism: A meta-analysis of randomized controlled trials. The International Journal of Neuropsychopharmacology, 8(2), 267-280.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 9 of 25
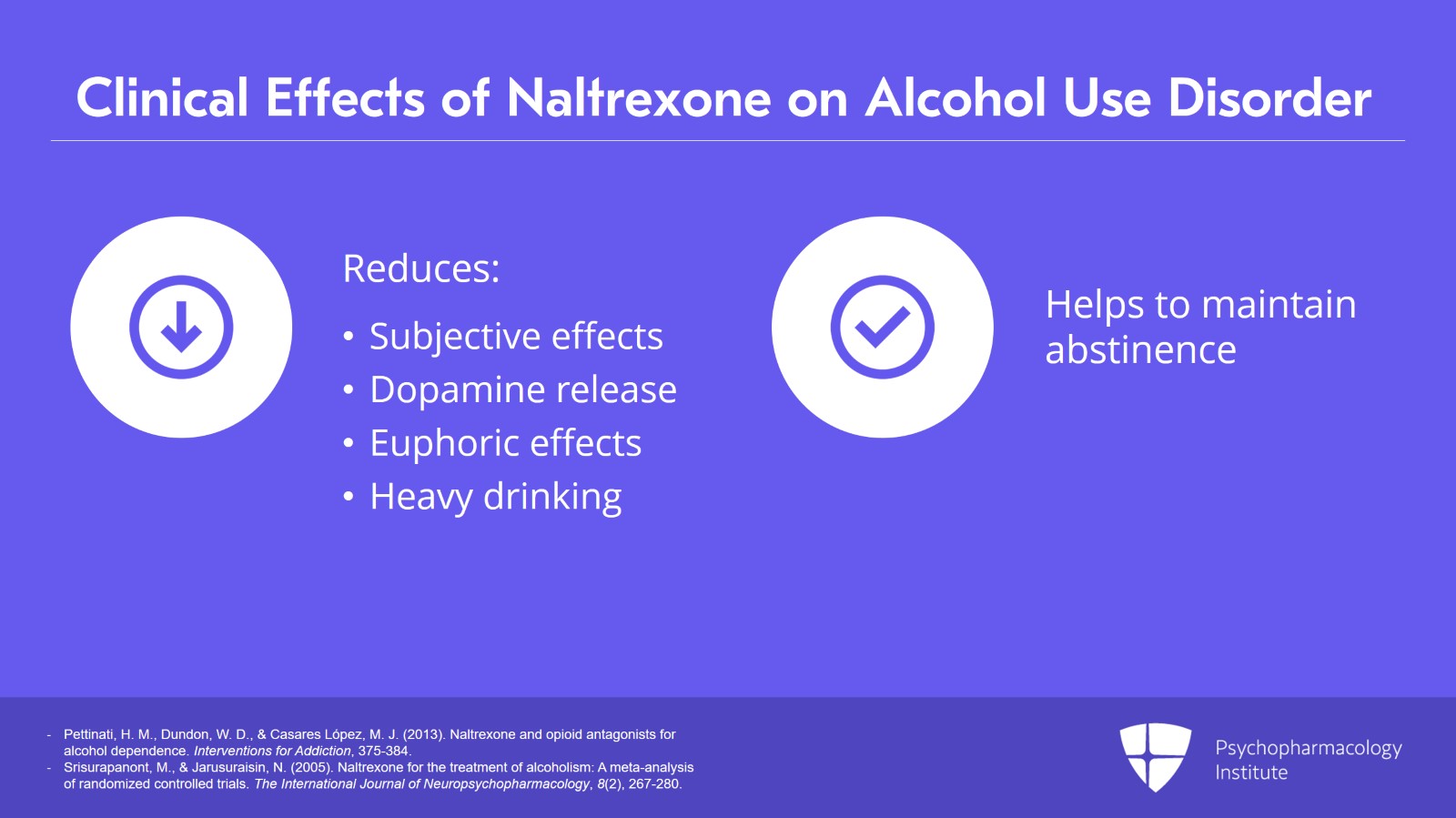
The main clinical effect of naltrexone is that it reduces the subjective effects of alcohol caused by the net reduction in the dopamine release from alcohol. The reason why this works is that when patients have their first drink, it becomes subsequently harder to say no to the second drink. After the second drink, saying no to the third is even harder and harder. There's a positive reinforcement. Naltrexone reduces the euphoric effects of alcohol such that it makes it easier to put down the second drink or the third drink. So it really seems to help reduce heavy drinking days but also has an effect on the ability of the individual to maintain abstinence if they're trying not to drink at all. So the overall evidence base is that it does help reduce heavy drinking, it does help delay any drinking. And then overall, it can, again, the big impact is on reduction in heavy drinking.
References:
- Pettinati, H. M., Dundon, W. D., & Casares López, M. J. (2013). Naltrexone and opioid antagonists for alcohol dependence. Interventions for Addiction, 375-384.
- Srisurapanont, M., & Jarusuraisin, N. (2005). Naltrexone for the treatment of alcoholism: A meta-analysis of randomized controlled trials. The International Journal of Neuropsychopharmacology, 8(2), 267-280.
Slide 10 of 25
The evidence is really strongly supportive of naltrexone impacting heavy drinking days but really it's considered appropriate for patients who are wanting to cut down or maintain their abstinence. And it's okay to start naltrexone even if the patient is still drinking. They don't have to first attain abstinence. But the overall benefit of naltrexone seems to be better if the patient is first able to attain abstinence for at least a couple days. Four days is sort of the cutoff.
References:
- Pettinati, H. M., Dundon, W. D., & Casares López, M. J. (2013). Naltrexone and opioid antagonists for alcohol dependence. Interventions for Addiction, 375-384.
- Srisurapanont, M., & Jarusuraisin, N. (2005). Naltrexone for the treatment of alcoholism: A meta-analysis of randomized controlled trials. The International Journal of Neuropsychopharmacology, 8(2), 267-280.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 11 of 25
But whenever the patient is willing to start in my mind is actually okay. And even if the goal is to cut back, like I find that to be a still reasonable initial goal, they may not be the appropriate goal in the longer term, but any reduction in drinking has health benefits and so I will never turn away a patient to say the only appropriate treatment goal is abstinence. Success in reduction in drinking actually may lead for the patient to be more confident in aiming for abstinence. Any reduction in the right direction is something that I would fully support. And if medications would help to do that, that's in my mind a good thing.
References:
- Pettinati, H. M., Dundon, W. D., & Casares López, M. J. (2013). Naltrexone and opioid antagonists for alcohol dependence. Interventions for Addiction, 375-384.
- Srisurapanont, M., & Jarusuraisin, N. (2005). Naltrexone for the treatment of alcoholism: A meta-analysis of randomized controlled trials. The International Journal of Neuropsychopharmacology, 8(2), 267-280.
Slide 12 of 25
There's naltrexone oral but there's also the injectable naltrexone which is a once-a-month medication. That's a gluteal IM injection. And it's considered to be more effective than the p.o. version. Overall, the total number of patients using this is relatively small so the evidence base is not as definitive but for many patients, just a once-a-month injection is much more convenient. And unlike the p.o. version, it has some signal that it really may support abstinence and not just reduction in heavy drinking days. So either is really a viable option for patients with alcohol use disorder. The oral or the intramuscular naltrexone, both are quite appropriate.
References:
- Gastfriend, D. R. (2011). Intramuscular extended-release naltrexone: Current evidence. Annals of the New York Academy of Sciences, 1216(1), 144-166.
- Pettinati, H. M., Dundon, W. D., & Casares López, M. J. (2013). Naltrexone and opioid antagonists for alcohol dependence. Interventions for Addiction, 375-384.

Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 13 of 25
There are times when clinicians utilize naltrexone as a p.r.n. medication to use it only during high-risk situations. I've had patients who don't use naltrexone regularly. But if they're going to a celebration or a party and they know there'll be alcohol around, they don't want to sort of drink at all or if they do end up drinking they want to minimize it, so depending on the situation, there are times when I've recommended to patients that a p.r.n. use may be indicated. But there's very minimal research on this type of approach and the majority of research is really done in the context of regular daily dosing on naltrexone.
References:
- Gastfriend, D. R. (2011). Intramuscular extended-release naltrexone: Current evidence. Annals of the New York Academy of Sciences, 1216(1), 144-166.
- Pettinati, H. M., Dundon, W. D., & Casares López, M. J. (2013). Naltrexone and opioid antagonists for alcohol dependence. Interventions for Addiction, 375-384.

Slide 14 of 25
The next medication that's FDA approved is acamprosate. We don't have a good understanding of the mechanism but we think it's a glutamatergic antagonist and a GABA agonist that sort of modulates the GABA system and maybe normalizes the glutamatergic sort of excitation. There really are no drug-drug interactions that are known for acamprosate. The effects of acamprosate should kick in within a couple of days. It's not like you have to wait a couple weeks. The dose that's used is 666 mg three times a day.
References:
- Rösner, S., Hackl-Herrwerth, A., Leucht, S., Lehert, P., Vecchi, S., & Soyka, M. (2010). Acamprosate for alcohol dependence. Sao Paulo Medical Journal, 128(6), 379-379.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 15 of 25
Generally, well tolerated. The most common side effects are the GI distress and diarrhea that can occur. And the biggest contraindication is kidney failure as opposed to liver failure in naltrexone. And so individuals with low creatinine clearance, actually less than 30, will be an absolute contraindication for acamprosate.
References:
- Rösner, S., Hackl-Herrwerth, A., Leucht, S., Lehert, P., Vecchi, S., & Soyka, M. (2010). Acamprosate for alcohol dependence. Sao Paulo Medical Journal, 128(6), 379-379.
Slide 16 of 25
The main effect of acamprosate really seems to be in promoting and maintaining abstinence. It has an effect on reduction in heavy drinking days to some degree but probably the biggest impact is on really sustaining abstinence and maintaining that. The largest US trial for acamprosate called Project COMBINE actually failed to show acamprosate's efficacy over a placebo. But if you look at the overall evidence including all the different trials, all the European trials, actually acamprosate comes out even better than naltrexone. There are mixed findings. But overall evidence does support its use and so we would strongly encourage it.
References:
- Rösner, S., Hackl-Herrwerth, A., Leucht, S., Lehert, P., Vecchi, S., & Soyka, M. (2010). Acamprosate for alcohol dependence. Sao Paulo Medical Journal, 128(6), 379-379.
- Donovan, D. M., Anton, R. F., Miller, W. R., Longabaugh, R., Hosking, J. D., & Youngblood, M. (2008). Combined Pharmacotherapies and behavioral interventions for alcohol dependence (The combine study): Examination of Posttreatment drinking outcomes. Journal of Studies on Alcohol and Drugs, 69(1), 5-13.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 17 of 25
Just like with naltrexone, some period of abstinence prior to initiation seems to be a good thing. For example, after an inpatient withdrawal management or a clinical detox admission, acamprosate is a good medication to start. Even if it's a small effect, we shouldn't discount it. Abstinence is really hard even in motivated people. Even a small reduction in overall drinking, even a small, improvement in abstinence is actually a great thing especially from a public health perspective. Once you're able to sustain some abstinence that gets people much more confident they can do this over the longer term. And just like with naltrexone, even if the short-term goal is not complete abstinence, any change and any reduction in alcohol is something that I support. Also, for acamprosate, two tabs t.i.d. is a difficult, you know, regimen to maintain. I maintain some flexibility around it. You know, if they have some side effects, a reduction in dose to one tab t.i.d., or if they want to do b.i.d. dosing to three tabs b.i.d. So I think there are multiple ways to kind of dose this and I try to be flexible with patients.
References:
- Rösner, S., Hackl-Herrwerth, A., Leucht, S., Lehert, P., Vecchi, S., & Soyka, M. (2010). Acamprosate for alcohol dependence. Sao Paulo Medical Journal, 128(6), 379-379.
- Rösner, S., Leucht, S., Lehert, P., & Soyka, M. (2007). Acamprosate supports abstinence, Naltrexone prevents excessive drinking: Evidence from a meta-analysis with unreported outcomes. Journal of Psychopharmacology, 22(1), 11-23.
Slide 18 of 25
And so the final FDA-approved medication is disulfiram. It inhibits an enzyme that breaks down acetaldehyde, the acetaldehyde dehydrogenase. And the reason why this works is ethanol is metabolized into acetaldehyde by the alcohol dehydrogenase. And then this acetaldehyde is further broken down into acetate by the acetaldehyde dehydrogenase. Disulfiram blocks the second enzyme. This leads to the accumulation of acetaldehyde which causes a very unpleasant reaction, sometimes called a flushing reaction, nausea, headache, even hypotension. And it can be quite uncomfortable. It's usually not severe. It doesn't lead people to, typically end up in the emergency room. But it's aversive enough to really be a deterrent. And so this has been around for a long time and it is an FDA-approved medication. And relatively well tolerated at the target dose which is 250 mg once a day.
References:
- Krampe, H., & Ehrenreich, H. (2010). Supervised disulfiram as adjunct to psychotherapy in alcoholism treatment. Current Pharmaceutical Design, 16(19), 2076-2090.
- De Sousa, A. (2019). Disulfiram in the management of alcohol dependence. Disulfiram, 21-30.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 19 of 25
Historically, higher doses were utilized but the higher dose is more prone to cause cognitive problems like delirium or even psychosis. And therefore, the lower doses are recommended. Now, rarely, it can cause liver failure and so liver monitoring, just like naltrexone, is actually important. The reason why psychosis has been a problem is that disulfiram also inhibits another enzyme, dopamine beta-hydroxylase. And this is an enzyme that breaks down dopamine. And therefore, disulfiram can actually increase dopamine levels in the brain. This is actually another reason why disulfiram has been tried as a treatment for stimulant use disorders because in those situations dopamine may be helpful.
References:
- Krampe, H., & Ehrenreich, H. (2010). Supervised disulfiram as adjunct to psychotherapy in alcoholism treatment. Current Pharmaceutical Design, 16(19), 2076-2090.
- De Sousa, A. (2019). Disulfiram in the management of alcohol dependence. Disulfiram, 21-30.
Slide 20 of 25
Therefore, this medication is contraindicated in individuals with a psychotic disorder. And this is actually a frequent board-type exam question, the interaction of disulfiram and psychotic disorders.
References:
- Krampe, H., & Ehrenreich, H. (2010). Supervised disulfiram as adjunct to psychotherapy in alcoholism treatment. Current Pharmaceutical Design, 16(19), 2076-2090.
- De Sousa, A. (2019). Disulfiram in the management of alcohol dependence. Disulfiram, 21-30.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 21 of 25
Now, this is a medication where patient selection is important. You don't want patients who are very impulsive and are really unable to control their drinking despite taking medications because of the adverse reactions. And so typically, this is reserved for more motivated patients. And one approach that can really improve the outcomes of disulfiram is to combine Behavioral Couples Therapy where the patient's spouse or family member actually administers the disulfiram each day to create this sort of accountability. And so for motivated patients or patients where you can incorporate Behavioral Couples approaches, this is actually a viable option to consider.
References:
- Krampe, H., & Ehrenreich, H. (2010). Supervised disulfiram as adjunct to psychotherapy in alcoholism treatment. Current Pharmaceutical Design, 16(19), 2076-2090.
Slide 22 of 25
Now, overall, these are sort of the FDA-approved medications and are considered first line. But because of patient selection and other issues, naltrexone and acamprosate really are the two sort of go-to medications for alcohol use disorder. There are many patient factors that you would take into account — patient preference prior response to these medications, contraindications and comorbid conditions. But in reality, I always tell people, whichever medication the patient is willing to take is the best one because that's what they're going to take. And again, any help in recovery is I think a good thing and so we should utilize them where appropriate.
References:
- Saitz, R. (2014). Medications for alcohol use disorders. JAMA, 312(13), 1349.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 23 of 25
So key points for this section are naltrexone's main effects are to reduce heavy drinking days but also to help promote abstinence and reducing cravings. Caution for those with liver dysfunction.
Slide 24 of 25
Acamprosate, another FDA-approved medication, can promote abstinence and reduce cravings. Without any drug-drug interactions, it's a fairly safe medication to use but caution in those with kidney dysfunction. Disulfiram is also a viable option but patient selection for those who are highly motivated is actually quite important.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 25 of 25

