
Slides and Transcript
Slide 1 of 8
Video 9 of the Algorithm for the Psychopharmacology of Major Depression from the Harvard South Shore Psychopharmacology Algorithm Project. We are working our way through the main algorithm for major depression in outpatients and the few remaining inpatients that didn’t have severe melancholia where you would be thinking of an antidepressant. In the previous video, we talked about the first trial and what we recommend for the first antidepressant. And now, we’re at the second trial. The first one has failed. And what are we going to do next? One of the toughest decisions in psychopharmacology because there’s such a huge amount of study of things that you could use after a failed trial but almost no direct comparisons of one thing with another.
Slide 2 of 8
So here’s how we approach it. First, review diagnosis again as you should after every failed trial for anything. If you think it’s unipolar depression but it’s bipolar, you could be wasting a lot of time or worse in treating this patient. So recheck your diagnosis after each failed trial. Significant others, by the way, may have better insight into the occurrence of discrete episodes of hypomania or mania that are occurring. So getting permission to and then checking with others who know the patient well may help understand why your treatments aren’t working and lead you to a correct diagnosis.
References:
- Altshuler, L. L., Post, R. M., Hellemann, G., Leverich, G. S., Nolen, W. A., Frye, M. A., … & Sugar, C. A. (2009). Impact of antidepressant continuation after acute positive or partial treatment response for bipolar depression: a blinded, randomized study. Journal of Clinical Psychiatry, 70(4), 450.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 8
Now, as I said in video 8, many have wondered if it’s better to switch or augment after the first failed trial in major depression although there is little evidence.
And perhaps the best study was STAR*D that compared patients who chose a switch for their second trial versus a group who chose augmentation and they matched those patients to have similar demographics and severity. They found an odds ratio of slightly better results with augmentation of 1.1 which was not statistically or clinically significant. So therefore, in this algorithm as in STAR*D, we let the patient decide if he/she wants an augmentation or a switch. We offer four choices for switching, what we think are reasonable well-established choices and four for augmentation which we think are among the best of those. And then the patient will sometimes prefer an option with fewer studies maybe that show efficacy in order to have the minimal side effects of them as opposed to picking maybe an FDA-approved option that has had many studies supporting efficacy although not better than other treatments but with considerable side effects. The best example of that would be the second-generation or atypical antipsychotics. Some of which are FDA approved but they have a big side effect burden.
References:
- Bschor, T., & Baethge, C. (2010). No evidence for switching the antidepressant: systematic review and meta‐analysis of RCTs of a common therapeutic strategy. Acta Psychiatrica Scandinavica, 121(3), 174-179.
- Papakostas, G. I., Fava, M., & Thase, M. E. (2008). Treatment of SSRI-resistant depression: a meta-analysis comparing within-versus across-class switches. Biological psychiatry, 63(7), 699-704.

Slide 4 of 8
So let’s go over our options. First, we have the switching options. We have four basic choices here. The first is to switch to one of the agents we recommended for the first trial that you didn’t try yet. So that’s either sertraline, escitalopram or bupropion. There have been studies showing up to 70% response rates after two or three consecutive monotherapy trials.
No significant difference has been found for switching within or between classes of antidepressants in two big meta-analyses. So you could do a different SSRI or you could switch to a different class like bupropion.
Now, the second switch option is to switch instead one of our three to a dual-action agent, something inhibiting both norepinephrine and serotonin reuptake. And here, the choices would be venlafaxine or mirtazapine.
There are some reports favoring switching to these agents. They’re mostly funded by their manufacturers, however, In STAR*D, there was an option of switching to venlafaxine. There was a numerical trend in favor of it over the SSRI switch. It was 25% remission on switch to venlafaxine, only 18% on sertraline switch and 21% on bupropion switch. That was not statistically significant but it’s a slight trend. The downside of venlafaxine is it can elevate the blood pressure, has more severe discontinuation syndromes, more GI side effects and more overdose fatalities. The mirtazapine switch is another option. It may work faster than other antidepressants according to some reviews but not better by 12 weeks. Weight gain must be actively monitored. There are rare cases of agranulocytosis.
References:
- Souery, D., Serretti, A., Calati, R., Oswald, P., Massat, I., Konstantinidis, A., … & Lecrubier, Y. (2011). Switching antidepressant class does not improve response or remission in treatment-resistant depression. Journal of clinical psychopharmacology, 31(4), 512-516.

Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 8
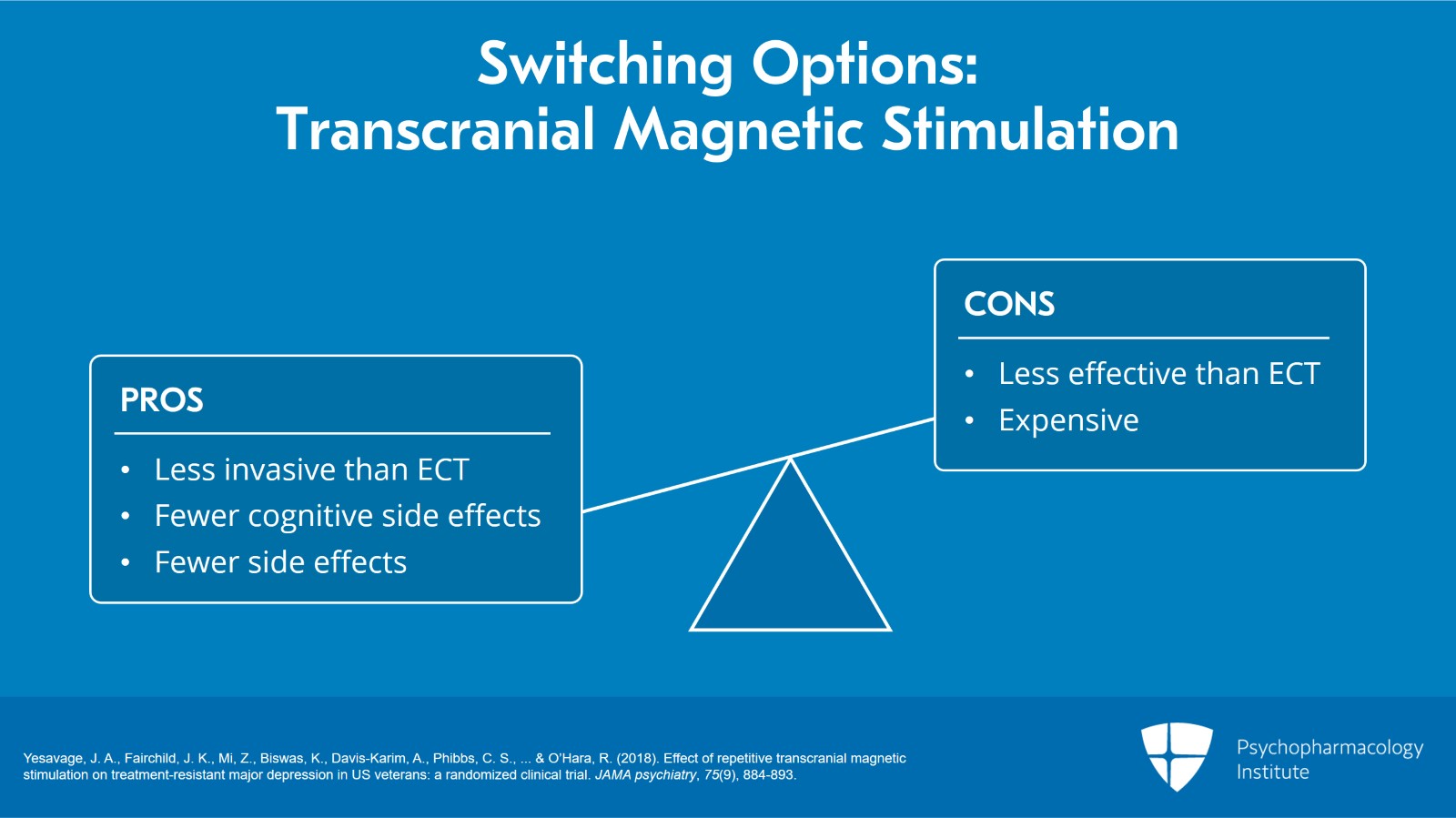
The third switch option is switching to regional transcranial magnetic stimulation.
It’s less invasive,
better cognitive side effect profile
but less effective than ECT
and basically has very few side effects.
Very expensive though but some people can afford it.
The FDA has approved rTMS after you have failed one medication trial but not two. Did you know that?
The data that was presented to the FDA for people who had failed two antidepressants didn’t show any difference from sham. So the FDA approved it only if you’ve had one trial.
References:
- Yesavage, J. A., Fairchild, J. K., Mi, Z., Biswas, K., Davis-Karim, A., Phibbs, C. S., … & O’Hara, R. (2018). Effect of repetitive transcranial magnetic stimulation on treatment-resistant major depression in US veterans: a randomized clinical trial. JAMA psychiatry, 75(9), 884-893.
Slide 6 of 8
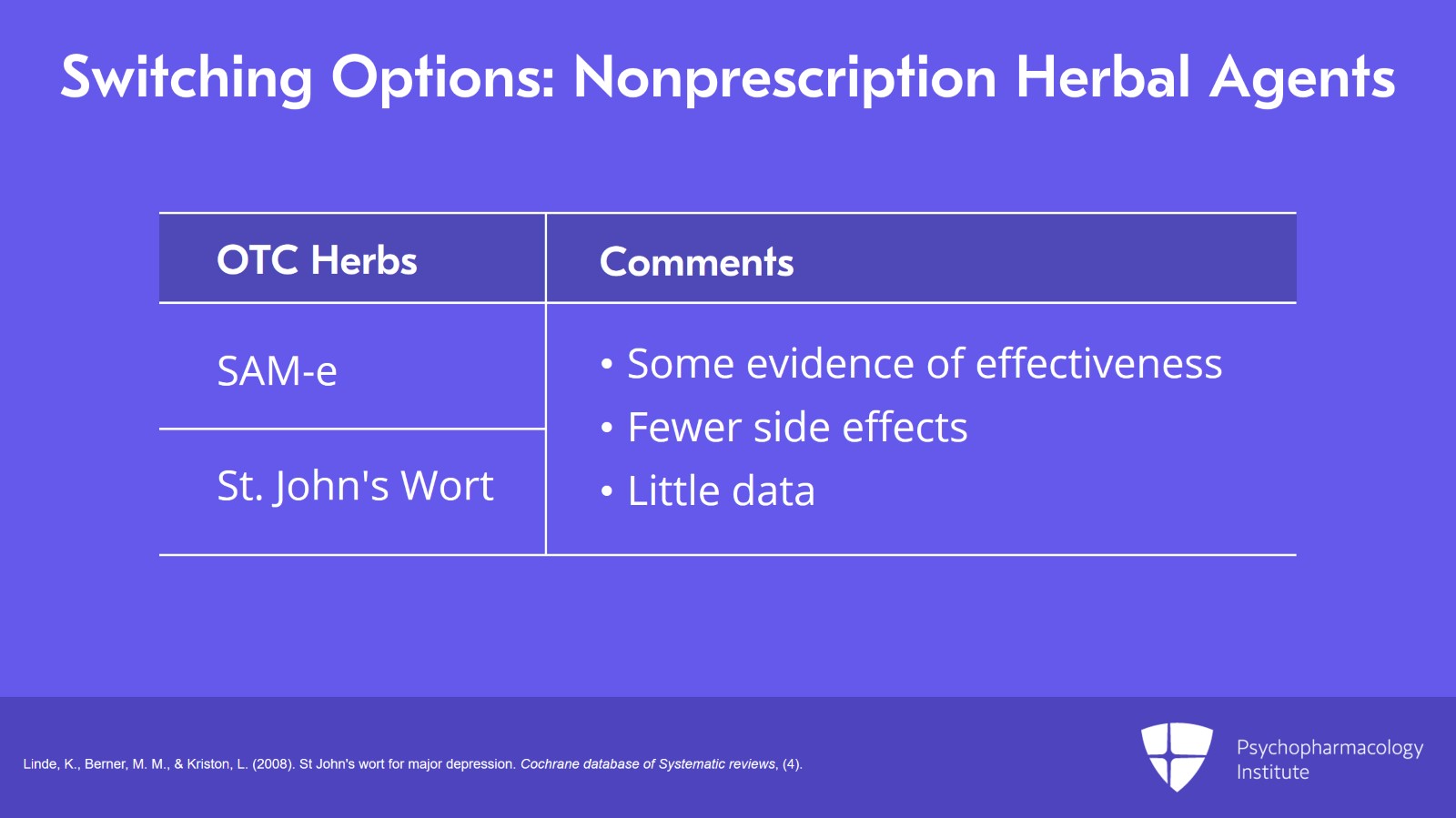
And finally, the fourth switch option is a switch to an over-the-counter non-prescription herbal or vitamin-like agent.
And in that category, we offer two that had decent evidence of effectiveness, S-adenosyl methionine or SAM-e or St. John’s wort.
They have fewer side effects than antidepressants and the patient may want to give one of them a try even though they don’t have a lot of data.
References:
- Linde, K., Berner, M. M., & Kriston, L. (2008). St John's wort for major depression. Cochrane database of Systematic reviews, (4).
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 8
So in summary, the key points of this video.
After the first failed trial of an antidepressant for major depression in this group of patients we have been discussing, let the patient decide if he/she wants to switch or augment that antidepressant. This was what was done with quite useful results in the STAR*D Study and we adopted it as a strategy for use in the algorithm.
There are four choices that we offer for switching and then four for augmentation. Each has its advantages and disadvantages. We recommend suggesting all or perhaps some of the four. And those were:
Choosing another one of the node 4 choices for first-line treatment, namely, sertraline, escitalopram or bupropion.
The second choice could be a dual-action agent, venlafaxine or mirtazapine.
Third would be transcranial magnetic stimulation or RTMS. It’s a reasonable and FDA-approved option for people who have failed one antidepressant trial but not approved if they’ve been given two or more.
And finally, S-adenosyl methionines known as SAM-e or St. John’s wort has significant evidence of effectiveness in major depression to make them worthy of consideration for a person who’s looking for something with practically no side effects and is easy to obtain.
We will discuss the augmentation choices in the next video.
Slide 8 of 8
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
