
Transcript
BPSD tends to occur because of a complex interaction between anatomical, functional, and biochemical changes that occur in the brain of individuals with dementia.
The presence of certain genes can predispose individuals to develop BPSD. An individual’s premorbid personality may also contribute to the emergence of certain types of behavioral symptoms in individuals with dementia.
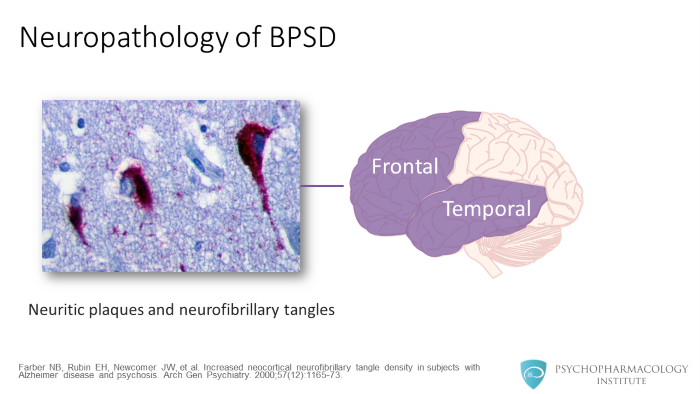
Let’s talk a little bit more in detail of some of the neurobiological changes that you see in individuals with dementia. The presence of neuritic plaques and neurofibrillary tangles in the frontal and temporal cortices are associated with behavioral symptoms, especially apathy.
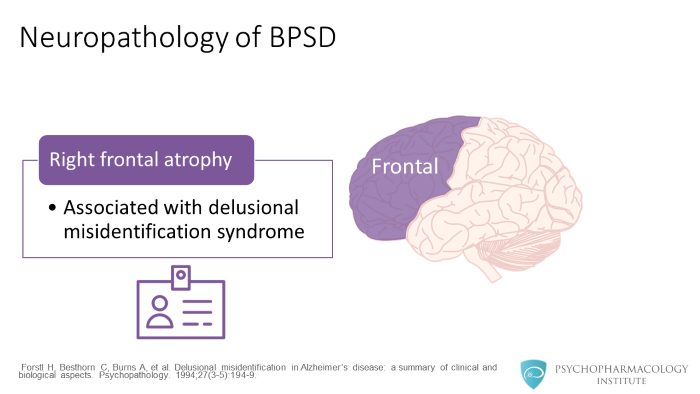
Right frontal lobe atrophy is associated with delusional misidentification syndromes.
Frontal, temporal, parietal cortical dysfunction is associated with psychotic symptoms in individuals with dementia.
Researchers have found that greater EEG delta-power over the right hemisphere is associated with greater delusional misidentification syndromes.
Some of the neurochemical changes associated with individuals who have BPSD include: damage to the cholinergic neurons (especially in the frontal and the temporal cortices) and adrenergic and serotonergic system abnormalities in these individuals.
There are high levels of norepinephrine in the substantia nigra and lower levels of serotonin in the presubiculum that are associated with psychotic symptoms.
There is also genetic correlation with behavioral and psychological symptoms of dementia. Depression tends to be more common in first-degree relatives of individuals who have depression. Heritability for psychotic symptoms varies between 30 and 61%.
The presence of APOE4 allele is associated with earlier onset of psychotic symptoms. The presence of APOE2 allele is associated with depressive symptoms. Those individuals with dementia who are homozygotes for APOE4 allele may have greater levels of disorientation, agitation, and motor symptoms. Anxiety and sleep disorders are more frequently seen in individuals who are homozygotes for APOE3 allele.
5-HT2A receptor polymorphism is associated with greater visual and auditory hallucinations, hyperphagia, and aggression in individuals with dementia. Dopamine receptor polymorphisms are associated with psychosis and aggression.
High level of premorbid neuroticism is associated with greater onset of depressive symptoms in individuals with dementia.
References
- Farber NB, Rubin EH, Newcomer JW, et al. Increased neocortical neurofibrillary tangle density in subjects with Alzheimer disease and psychosis . Arch Gen Psychiatry. 2000;57(12):1165-73.
- Forstl H, Besthorn C, Burns A, et al. Delusional misidentification in Alzheimer’s disease: a summary of clinical and biological aspects . Psychopathology. 1994;27(3-5):194-9
- Mentis MJ, et al. Abnormal brain glucose metabolism in the delusional misidentification syndromes: a positron emission tomography study in Alzheimer disease. Biol Psychiatry . 1995;38(7):438-49.
- Cummings JL, Back C. The cholinergic hypothesis of neuropsychiatric symptoms in Alzheimer’s disease . Am J Geriatr Psychiatry. 1998;6(2 Suppl 1):S64-78
- Zubenko GS, Moossy J, Martinez J, et al: Neuropathologic and neurochemical correlates of psychosis in primary dementia . Arch Neurol. 1991; 48:619–624.
- Bacanu SA, Devlin B, Chowdari KV, et al. Heritability of psychosis in Alzheimer disease . Am J Geriatr Psychiatry. 2005;13(7):624-7.
- Ballard C, Massey H, Lamb H, et al. Apolipoprotein E: non-cognitive symptoms and cognitive decline in late onset Alzheimer’s disease . J Neurol Neurosurg Psychiatry. 1997;63(2):273-4
- Sukonick DL, Pollock BG, Sweet RA, et al. The 5-HTTPR*S/*L polymorphism and aggressive behavior in Alzheimer disease . Arch Neurol. 2001;58(9):1425-8
- Meins W, Frey A, Thiesemann R. Premorbid personality traits in Alzheimer’s disease: do they predispose to noncognitive behavioral symptoms? Int Psychogeriatr . 1998;10(4):369-78
