Slides and Transcript
Slide 1 of 23
In section 4, we’re going to talk about medication-induced tremors.
Slide 2 of 23
So medication-induced tremors are usually postural or kinetic tremors, and less often resting tremor.
References:
- Baizabal-Carvallo, J. F., & Morgan, J. C. (2022). Drug-induced tremor, clinical features, diagnostic approach and management. Journal of the Neurological Sciences, 435, Article 120192. https://doi.org/10.1016/j.jns.2022.120192
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 23
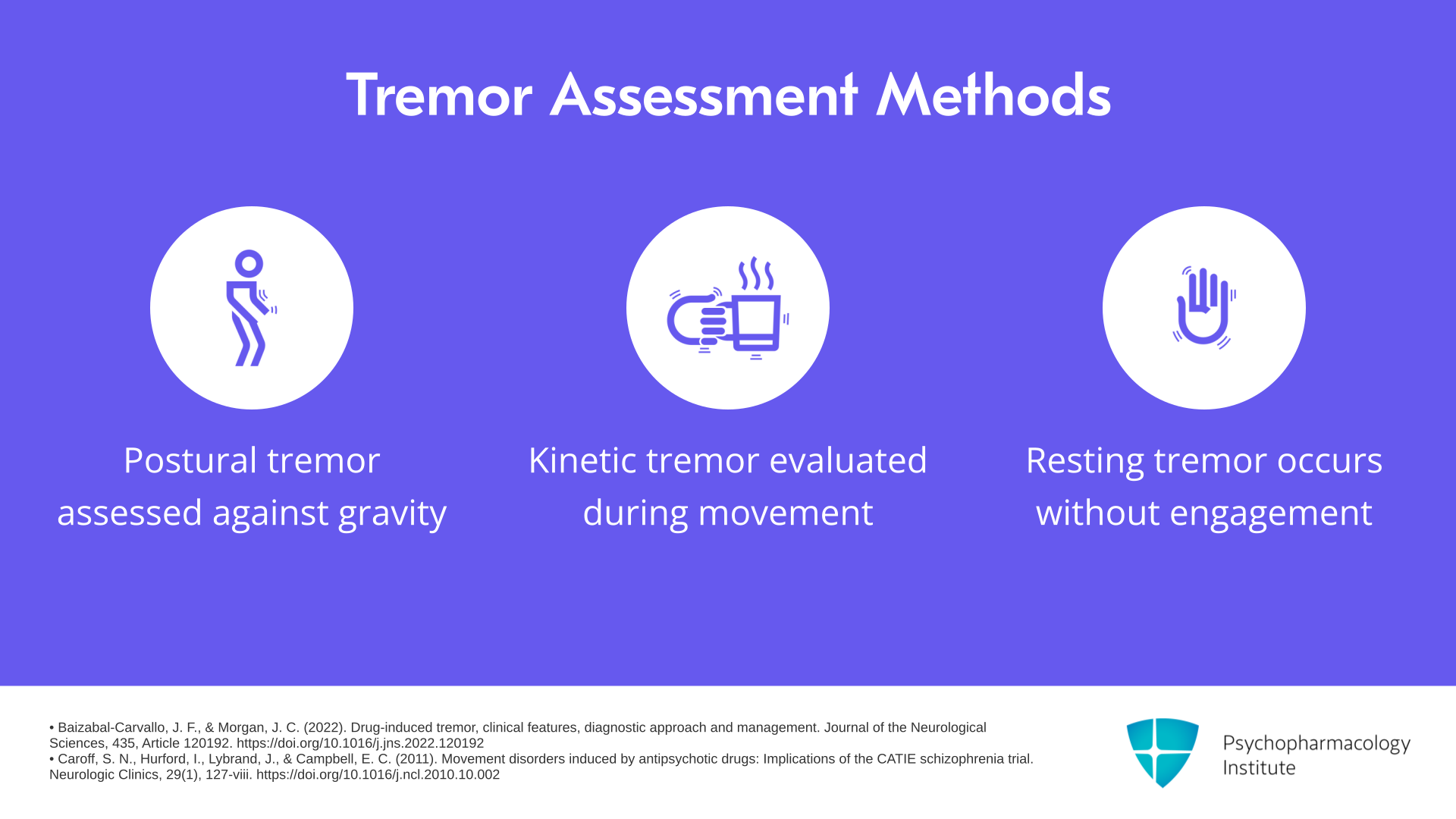
Just to refresh our memories, postural tremor is assessed when the limb is unsupported against gravity, kinetic or action tremors are assessed by having the limb move through space, and then resting tremor is when the limb is not engaged in voluntary movement, supported against gravity. That’s how you assess these.
References:
- Baizabal-Carvallo, J. F., & Morgan, J. C. (2022). Drug-induced tremor, clinical features, diagnostic approach and management. Journal of the Neurological Sciences, 435, Article 120192. https://doi.org/10.1016/j.jns.2022.120192
- Caroff, S. N., Hurford, I., Lybrand, J., & Campbell, E. C. (2011). Movement disorders induced by antipsychotic drugs: Implications of the CATIE schizophrenia trial. Neurologic Clinics, 29(1), 127-viii. https://doi.org/10.1016/j.ncl.2010.10.002
Slide 4 of 23
Risk factors for medication-induced tremors are older age, which is the most significant risk factor. People with liver failure tend to be more susceptible to medication-induced tremor. People with other metabolic abnormalities, central nervous system pathology like stroke or traumatic brain injury tend to be a little more vulnerable to these.
References:
- Baizabal-Carvallo, J. F., & Morgan, J. C. (2022). Drug-induced tremor, clinical features, diagnostic approach and management. Journal of the Neurological Sciences, 435, Article 120192. https://doi.org/10.1016/j.jns.2022.120192
- Morgan, J. C., Kurek, J. A., Davis, J. L., & Sethi, K. D. (2017). Insights into pathophysiology from medication-induced tremor. Tremor and Other Hyperkinetic Movements, 7, 442. https://doi.org/10.7916/D8FJ2V9Q
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 23
Clinically, you want to look for a temporal association between the tremor onset or worsening with medication initiation or titration. So usually with most of the medications that cause tremor, the higher the dose, the worse the tremor. So there’s almost a dose-response relationship between the medication dosing and the severity of the tremor.
References:
- Morgan, J. C., Kurek, J. A., Davis, J. L., & Sethi, K. D. (2017). Insights into pathophysiology from medication-induced tremor. Tremor and Other Hyperkinetic Movements, 7, 442. https://doi.org/10.7916/D8FJ2V9Q
Slide 6 of 23
Sometimes, the mechanism can be enhanced physiologic tremor. So the stretch receptors in our musculature produce tremor rhythmically to some degree for all of us based on many factors but medications like lithium, for instance, are thought to enhance the sensitivity of these stretch receptors and thereby sort of enhance or worsen the physiologic tremor. And so that’s the way some of these medications may be worsening a tremor that’s already there that most of us have.
References:
- Baizabal-Carvallo, J. F., & Morgan, J. C. (2022). Drug-induced tremor, clinical features, diagnostic approach and management. Journal of the Neurological Sciences, 435, Article 120192. https://doi.org/10.1016/j.jns.2022.120192
- Morgan, J. C., Kurek, J. A., Davis, J. L., & Sethi, K. D. (2017). Insights into pathophysiology from medication-induced tremor. Tremor and Other Hyperkinetic Movements, 7, 442. https://doi.org/10.7916/D8FJ2V9Q
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 23
But you do need to exclude other causes of tremor, such as idiopathic movement disorders. If you’re working with the elderly population, the highest prevalence of Parkinson’s is in the sixth decade. Ataxias are common essential tremor.
References:
- Morgan, J. C., Kurek, J. A., Davis, J. L., & Sethi, K. D. (2017). Insights into pathophysiology from medication-induced tremor. Tremor and Other Hyperkinetic Movements, 7, 442. https://doi.org/10.7916/D8FJ2V9Q
- Bötzel, K., Tronnier, V., & Gasser, T. (2014). The differential diagnosis and treatment of tremor. Deutsches Arzteblatt International, 111(13), 225-236. https://doi.org/10.3238/arztebl.2014.0225
Slide 8 of 23
Thyroid disorders can cause tremor, especially hyperthyroidism. Low blood sugar, hypoglycemia is another cause of tremor. And then many withdrawal states can cause tremor. So alcohol withdrawal, benzodiazepine withdrawal can cause this.
References:
- Morgan, J. C., Kurek, J. A., Davis, J. L., & Sethi, K. D. (2017). Insights into pathophysiology from medication-induced tremor. Tremor and Other Hyperkinetic Movements, 7, 442. https://doi.org/10.7916/D8FJ2V9Q
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 9 of 23
What are some of the most common medications that cause tremor? Many of the antidepressants, especially at higher doses. Mood stabilizers especially lithium are known to cause a tremor. Valproic acid is another one that causes tremor. So antiarrhythmic medications, beta-adrenergic agonists are associated with tremor.
References:
- Arbaizar, B., Gómez-Acebo, I., & Llorca, J. (2008). Postural induced-tremor in psychiatry. Psychiatry and Clinical Neurosciences, 62(6), 638-645. https://doi.org/10.1111/j.1440-1819.2008.01877.x
Slide 10 of 23
Many of the chemotherapies that are used can cause tremor, many drugs of abuse, stimulants, for instance, gastrointestinal drugs. Many hormone therapies can be associated with tremor. Immunosuppressants. Methylxanthines are another one.
References:
- Arbaizar, B., Gómez-Acebo, I., & Llorca, J. (2008). Postural induced-tremor in psychiatry. Psychiatry and Clinical Neurosciences, 62(6), 638-645. https://doi.org/10.1111/j.1440-1819.2008.01877.x
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 11 of 23
And then dopamine blockers, so in this category are antipsychotics, certain antiemetics and dopamine depleters, the VMAT2 inhibitors. The vesicular membrane transport protein that brings dopamine to the synapse. And if you’re interfering with that process, you’re de facto depleting the intrasynaptic dopamine. So any way that you get to that dysregulated dopamine state, you can cause tremor.
References:
- Morgan, J. C., Kurek, J. A., Davis, J. L., & Sethi, K. D. (2017). Insights into pathophysiology from medication-induced tremor. Tremor and Other Hyperkinetic Movements, 7, 442. https://doi.org/10.7916/D8FJ2V9Q
- Arbaizar, B., Gómez-Acebo, I., & Llorca, J. (2008). Postural induced-tremor in psychiatry. Psychiatry and Clinical Neurosciences, 62(6), 638-645. https://doi.org/10.1111/j.1440-1819.2008.01877.x
Slide 12 of 23
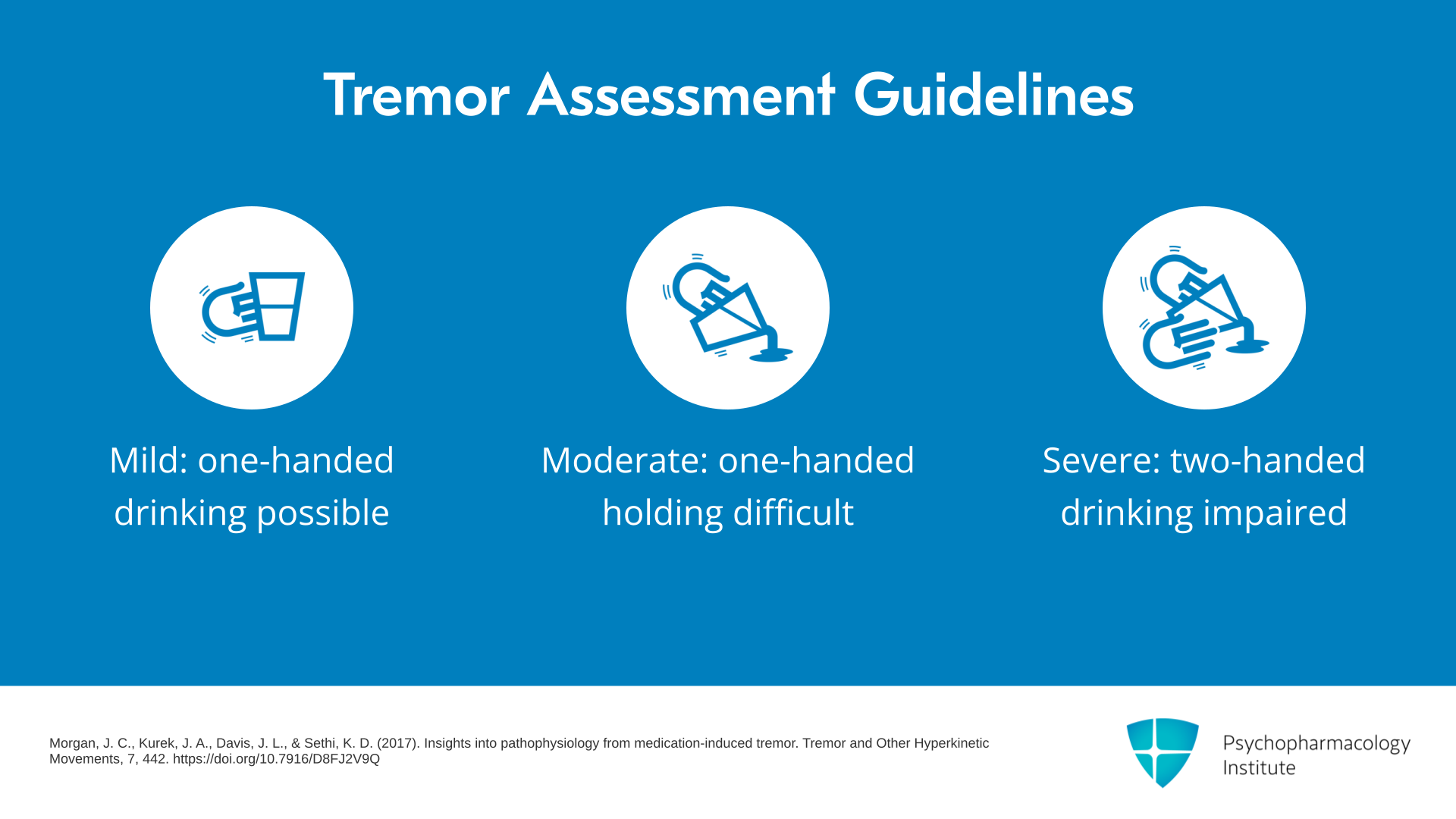
How do you treat a medication-induced tremor? Well, although there are several assessments for grading severity of tremor, there’s probably a more simple heuristic in terms of determining when to treat. If you can drink from a glass one-handed, that tremor is mild. And depending on the patient, you may or may not need or want to treat. A more moderate severity tremor is when holding a glass one-handed is difficult. And then severe is when drinking is difficult or maybe even impossible, even using two hands. So that’s a good rule of thumb to determine when to treat and how aggressively to treat.
References:
- Morgan, J. C., Kurek, J. A., Davis, J. L., & Sethi, K. D. (2017). Insights into pathophysiology from medication-induced tremor. Tremor and Other Hyperkinetic Movements, 7, 442. https://doi.org/10.7916/D8FJ2V9Q
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 13 of 23
Drug therapy is often required for moderate and severe tremors because now it’s interfering with function, especially if you can’t replace the causal agent. The symptom of interest is so disabling or distressing that you really can’t find another alternative.
References:
- Baizabal-Carvallo, J. F., & Morgan, J. C. (2022). Drug-induced tremor, clinical features, diagnostic approach and management. Journal of the Neurological Sciences, 435, Article 120192. https://doi.org/10.1016/j.jns.2022.120192
- Morgan, J. C., Kurek, J. A., Davis, J. L., & Sethi, K. D. (2017). Insights into pathophysiology from medication-induced tremor. Tremor and Other Hyperkinetic Movements, 7, 442. https://doi.org/10.7916/D8FJ2V9Q
Slide 14 of 23
So then the first-line treatment for tremor is really determined by potential side effects and tolerability of that individual patient. Beta-adrenergic blockers are typically well tolerated and used first line. So beta-blockers reduce the amplitude, but not the frequency of the tremor. Amplitude is the size of the tremor. And on average, about half of patients respond to some degree. So you got about a 50-50 response rate on beta-blockers, and you do need to push the dose.
References:
- Baizabal-Carvallo, J. F., & Morgan, J. C. (2022). Drug-induced tremor, clinical features, diagnostic approach and management. Journal of the Neurological Sciences, 435, Article 120192. https://doi.org/10.1016/j.jns.2022.120192
- Pal, P. K. (2011). Guidelines for management of essential tremor. Annals of Indian Academy of Neurology, 14(Suppl 1), S25–S28. https://doi.org/10.4103/0972-2327.83097
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 15 of 23
With propranolol, which is the one that’s recommended, you usually start at a low dose of 10 mg per day in divided doses. It’s got a fairly short half-life. But the therapeutic range in divided doses can be between 60 and 320 mg per day. So at the higher ranges especially, you have to watch out for side effects which can include fatigue, slowed heart rate, because it is a beta-blocker, and erectile dysfunction.
References:
- Baizabal-Carvallo, J. F., & Morgan, J. C. (2022). Drug-induced tremor, clinical features, diagnostic approach and management. Journal of the Neurological Sciences, 435, Article 120192. https://doi.org/10.1016/j.jns.2022.120192
- Pal, P. K. (2011). Guidelines for management of essential tremor. Annals of Indian Academy of Neurology, 14(Suppl 1), S25–S28. https://doi.org/10.4103/0972-2327.83097
Slide 16 of 23
Another option is primidone. Primidone at 75 mg at bedtime is usually a good place to start, and then you can increase until the tremor of interest has improved, or you’ve reached about 250 mg per day. The response rate is similar to that of the beta-blockers. Maybe about 50% of people will respond. It reduces the amplitude but not the frequency of the tremor. It’s a little more likely to cause side effects than the beta-blockers. You can get ataxia, sedation, vertigo, fatigue and nausea. So usually because of this higher risk of adverse effects, it’s considered second line.
References:
- Baizabal-Carvallo, J. F., & Morgan, J. C. (2022). Drug-induced tremor, clinical features, diagnostic approach and management. Journal of the Neurological Sciences, 435, Article 120192. https://doi.org/10.1016/j.jns.2022.120192
- Vogelnik Žakelj, K., Prezelj, N., Gregorič Kramberger, M., & Kojović, M. (2024). Mechanisms of tremor-modulating effects of primidone and propranolol in essential tremor. Parkinsonism & Related Disorders, 128, 107151. https://doi.org/10.1016/j.parkreldis.2024.107151
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 17 of 23
Gabapentin in doses between 1200 mg to 3600 mg per day is usually well tolerated. You do have to start low and increase rather slowly. So we say start around 400 mg. Side effects of gabapentin are dizziness, nausea, and sedation. It’s typically fairly well tolerated though, but only about 25% of patients respond. So although its tolerability is up there with the beta-blockers, its efficacy is about half of that.
References:
- Baizabal-Carvallo, J. F., & Morgan, J. C. (2022). Drug-induced tremor, clinical features, diagnostic approach and management. Journal of the Neurological Sciences, 435, Article 120192. https://doi.org/10.1016/j.jns.2022.120192
- Pourbala, H., Nahavandi, Z., Maghsoudlou, A., Farahani, M. G., Khallaghi, A., Izadi, S., Faizi, M., Ghaffari, M., & Esmaily, H. (2025). The impact of pregabalin and gabapentin on essential tremor: a systematic review and meta-analysis. Clinical Parkinsonism & Related Disorders, 13, 100381. https://doi.org/10.1016/j.prdoa.2025.100381
Slide 18 of 23
And then finally, topiramate started at about 25 mg per day, with a therapeutic range between 200 and 400 per day is proven to have modest efficacy in a large randomized controlled trial. However, topiramate is not as well tolerated as the other options due to paresthesia, word finding difficulty, nausea, somnolence, kidney stones and ciliary edema. It can cause blurred vision. So tolerability is the limiter for topiramate, but if they failed all these others, topiramate may be a viable option.
References:
- Baizabal-Carvallo, J. F., & Morgan, J. C. (2022). Drug-induced tremor, clinical features, diagnostic approach and management. Journal of the Neurological Sciences, 435, Article 120192. https://doi.org/10.1016/j.jns.2022.120192
- Connor, G. S., Edwards, K., & Tarsy, D. (2002). A double-blind placebo-controlled trial of topiramate treatment for essential tremor. Neurology, 59(1), 132-134. https://doi.org/10.1212/wnl.59.1.132
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 19 of 23
Benzodiazepines as a class have mixed evidence. Alprazolam produced about 34% response rate at doses between 0.75 mg and 3 mg daily, while clonazepam has variable results, sometimes benefiting head, trunk, and voice tremors in doses between 0.5 mg and 6 mg daily, or making no appreciable difference and so really kind of mixed profile of response.
References:
- Baizabal-Carvallo, J. F., & Morgan, J. C. (2022). Drug-induced tremor, clinical features, diagnostic approach and management. Journal of the Neurological Sciences, 435, Article 120192. https://doi.org/10.1016/j.jns.2022.120192
- Zhang, J., Yan, R., Cui, Y., Su, D., & Feng, T. (2024). Treatment for essential tremor: a systematic review and Bayesian Model-based Network Meta-analysis of RCTs. EClinicalMedicine, 77, 102889. https://doi.org/10.1016/j.eclinm.2024.102889
Slide 20 of 23
And then all of these benzodiazepines, carry the risk of sedation, fatigue, dependence with chronic use, and in the elderly, it can cause cognitive impairment and falls.
References:
- Estevez-Fraga, C., Zeun, P., & López-Sendón Moreno, J. L. (2018). Current methods for the treatment and prevention of drug-induced parkinsonism and tardive dyskinesia in the elderly. Drugs & Aging, 35(11), 959-971. https://doi.org/10.1007/s40266-018-0590-y
- Zhang, J., Yan, R., Cui, Y., Su, D., & Feng, T. (2024). Treatment for essential tremor: a systematic review and Bayesian Model-based Network Meta-analysis of RCTs. EClinicalMedicine, 77, 102889. https://doi.org/10.1016/j.eclinm.2024.102889
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 21 of 23
Finally, for certain cases, botulinum toxin can improve tremor and this does it, focally, locally. It does cause muscle weakness as a primary effect, but that also can reduce the amplitude of the tremor and it has to be refreshed. You have to get a new botulinum injection every three to four months, but I’ve seen this used to good effect in some cases.
References:
- Liao, Y. H., Hong, C. T., & Huang, T. W. (2022). Botulinum toxin for essential tremor and hands tremor in the neurological diseases: A meta-analysis of randomized controlled trials. Toxins, 14(3), 203. https://doi.org/10.3390/toxins14030203
- Visser, I. M., Pitakpatapee, Y., van de Warrenburg, B., Helmich, R. C., Snijders, A. H., & Nijhuis, F. A. P. (2025). Botulinum toxin efficacy in upper limb tremor: A systematic review and meta-analysis. Movement Disorders Clinical Practice, 10, 10.1002/mdc3.70307. Advance online publication. https://doi.org/10.1002/mdc3.70307
Slide 22 of 23
So the key points for this section are that medication-induced tremors can be a side effect of several different classes of medication. So a history that includes an accurate timeline is important. You really have to know when something was started or increased to make that association. Tremors should be treated if it interferes with daily function. Remember the difference between mild, moderate, and severe in terms of holding a glass.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 23 of 23
Beta-blockers, primidone, gabapentin, benzodiazepines in decreasing order of evidence of efficacy may be helpful if the medication causing the tremor cannot be changed.