
Slides and Transcript
Slide 1 of 22
What can we do for the pharmacologic management of difficult-to-treat depression?
Slide 2 of 22
I think it always begins with a diagnostic reevaluation. One of the more common things is, this person has depression. But are there other factors? Could they have bipolar depression? Could there be some life circumstances that are keeping them from being better? When was the last time we did any blood work that could identify anemia or hypothyroidism or something like that?
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 22
The next one, assessing adherence and drug-drug interactions. Many people do not fill every prescription we give them for medication. Research has shown that asking people in a non-judgmental way about adherence such as saying something like, everyone misses pills once in a while. Thinking carefully, are there drug-drug interactions? It’s very helpful to reconsider that in the case of difficult-to-treat depression.
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Slide 4 of 22
Don’t rule out medicines for one previous failure. Consider all medication trials when they were done and then see about the appropriateness of using any of them in the current circumstance.
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 22
The person starts to improve and we feel hesitant like it’s not broken right now so I don’t want to change anything, I don’t want to discontinue the old medicine. We should have more courage in saying, they were on the old medicine for a long time. We made a decision to transition to a new medicine. Let’s carry on and get rid of something that we knew was there for years and wasn’t working. So discontinue non-beneficial medications.
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Slide 6 of 22
Of course we’re carefully monitoring symptoms but let’s be clear about what side effects may have been more subtle and not bothersome acutely but are more bothersome in the long term. And how is the person functioning? And what do we need to do to improve the functioning?
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 22
When you have clear problems with a person not really responding, you go through the basics. An initial approach might be to, if this medicine is tolerable and we’ve only used a low but therapeutic dose, maybe we can optimize the dose. CANMAT does not recommend always going on every medicine to the maximum dose but instead a couple of dose adjustments at least achieving moderate dosing would be appropriate and then it can be considered what to do next.
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Slide 8 of 22
What to do next could be determined by whether the person needs to switch or add an adjunct medication. Now, while we’re talking about medications, we should always be thinking about, is there a role for adding psychological treatments here? There are the first-line psychological treatments and it may be possible to add these even in a modest way such as digital tools. Adding that could help while the person is being optimized on medication.
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 9 of 22
So we have to keep these other principles in mind while we pursue the major question – do we add a new medicine or do we switch to another medicine altogether after we have optimized the dose at least once? So we would generally consider switching if it’s been the first antidepressant or the first antidepressant is not very well tolerated or there’s absolutely no response. That response we could quantify as saying, did their depression rating scale, their PHQ-9 report, did it show at least a 20-25% improvement or not? If there was no improvement, maybe the medicine is not worth sticking on.
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Slide 10 of 22
If the medicine you’re using now already is showing some benefit, then you want to build on that and that would allow us to think of adding adjuncts. In general, adjunct therapies will show some improvement within two weeks and definitely by four weeks. So that’s a bit faster than simply switching to another antidepressant. The adjunct treatments also can target specific residual symptoms particularly well so you can achieve benefit both for efficacy and side effect management.
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 11 of 22
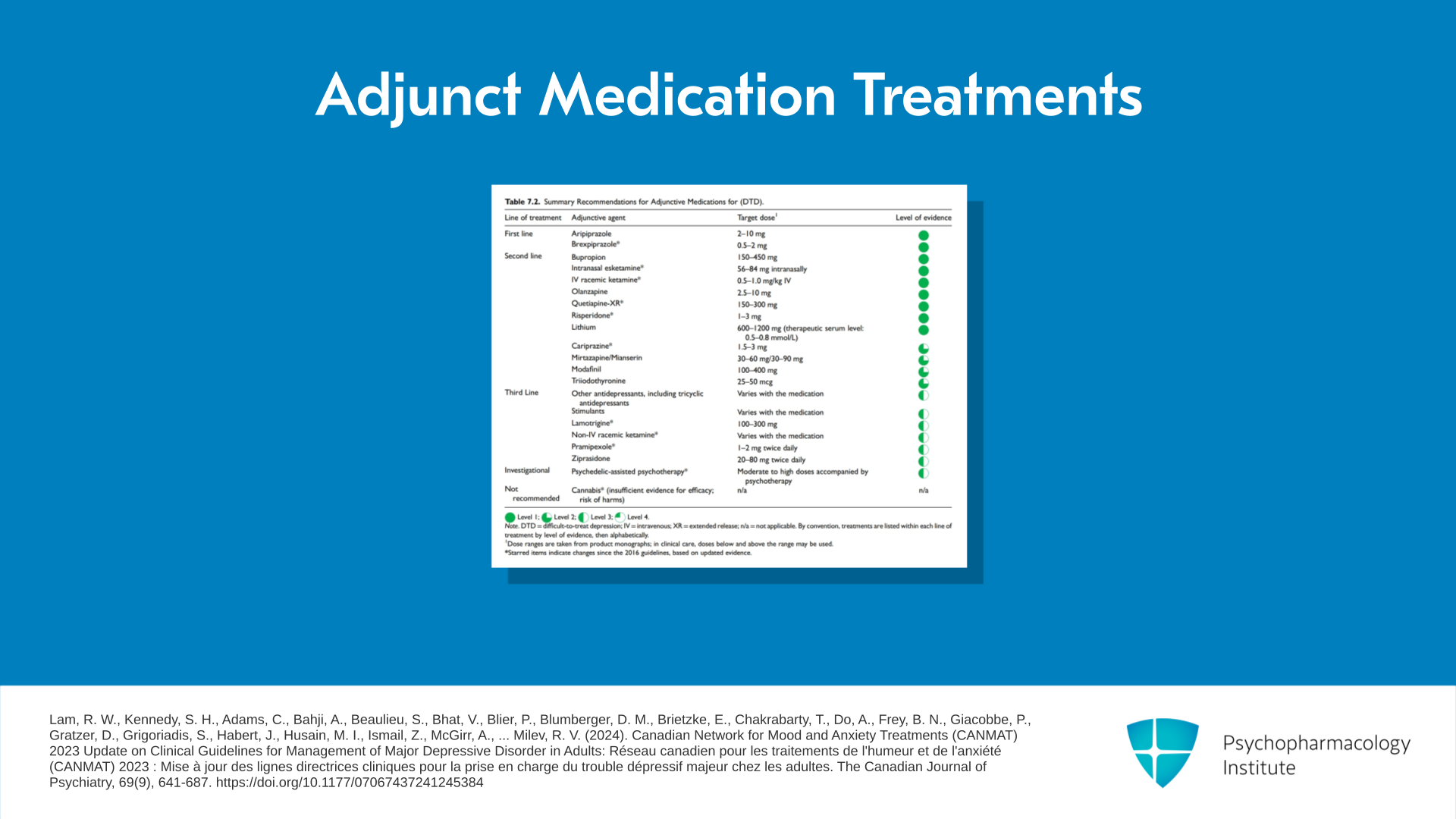
The medication treatments that can be used as adjunct agents are listed in the next table here.
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Slide 12 of 22
So we can see there are two first-line treatments – aripiprazole and brexpiprazole. In the historic research that was done with aripiprazole, 5 to 15 mg were typically used. More recent studies have shown that 2 to 5 mg are the appropriate doses for this. And in my own experience, 2 mg is the ideal dose. The doses that are there for brexpiprazole starting at 0.5 or 1 mg and possibly sitting or aiming at 2 and possibly going to 3.
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 13 of 22
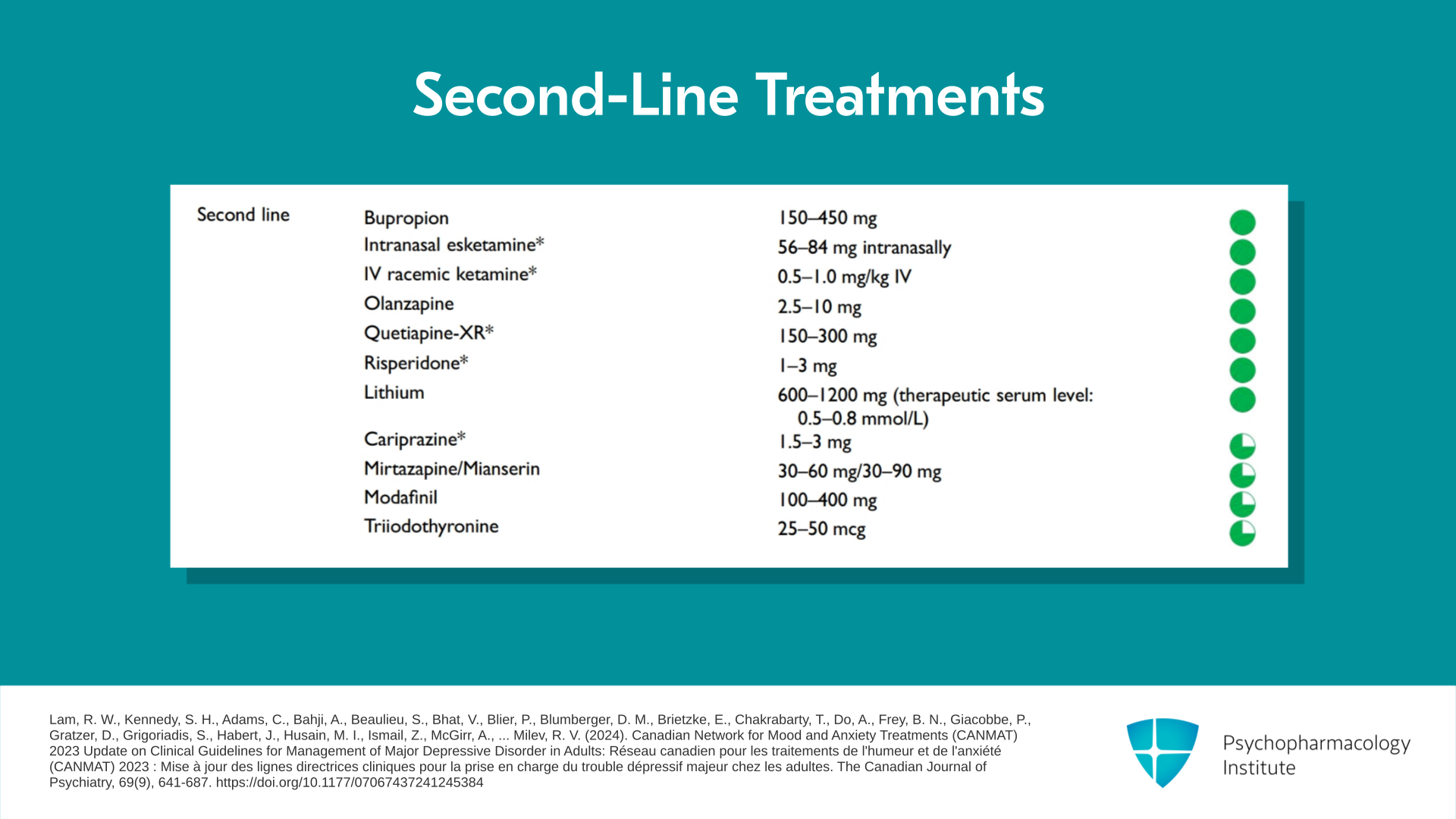
We can see there are a variety of second-line treatments which have a fully filled in green circle, meaning that they have first-line evidence. The reason they’re second line may be because of side effect concerns, accessibility, tolerability and so on. Among the things that are second line are the various forms of ketamine, esketamine intranasal or IV ketamine. Olanzapine which of course has significant metabolic and other side effects but is still useful. There’s quetiapine, Seroquel, which actually has been studied as an adjunct agent. There’s risperidone. And particularly of the newer agents, there’s cariprazine which is very promising and very simple to use and generally well tolerated and we think will likely be elevated to first-line status very soon.
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Slide 14 of 22
We’ve mentioned a lot of the augmentation agents are atypical antipsychotics. Atypical antipsychotics have a significant side effect burden particularly in the elderly and there are warnings about stroke risk in the elderly and so on. The extrapyramidal symptoms are particularly bothersome to patients in all age groups and the various other side effects that are associated with atypical antipsychotics can include weight gain and QTc issues and so forth.
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 15 of 22
The table does not include cariprazine at a dose of 1.5 mg per day with the possibility but not the necessity of raising the dose. I would really like to emphasize in the dosing that less may be more when we’re talking about augmentation agents.
References:
- Sachs, G. S., Yeung, P. P., Rekeda, L., Khan, A., Adams, J. L., & Fava, M. (2023). Adjunctive cariprazine for the treatment of patients with major depressive disorder: A randomized, double-blind, placebo-controlled phase 3 study. American Journal of Psychiatry, 180(3), 241-251. https://doi.org/10.1176/appi.ajp.20220504
Slide 16 of 22
In quetiapine, the ideal dose is actually 150 mg of the XR formulation. The original study suggested that an increase up to 300 mg could be used. But trying to get up to the 150 mg dose quickly is going to get you better results. And the dosing approach used in the studies is namely 50 mg at night for a couple of nights and then go directly to 150. Patients can be informed that they can go more slowly but if they want quicker results, it’s better to do it quickly rather than to do it slowly.
References:
- Bauer, M., Pretorius, H. W., Constant, E. L., Earley, W. R., Szamosi, J., & Brecher, M. (2009). Extended-release quetiapine as adjunct to an antidepressant in patients with major depressive disorder: results of a randomized, placebo-controlled, double-blind study. The Journal of Clinical Psychiatry, 70(4), 540-549. https://doi.org/10.4088/jcp.08m04629
- McIntyre, R. S., Muzina, D. J., Adams, A., Lourenco, M. T. C., Law, C. W. Y., Soczynska, J. K., Woldeyohannes, H. O., Nathanson, J., & Kennedy, S. H. (2009). Quetiapine XR efficacy and tolerability as monotherapy and as adjunctive treatment to conventional antidepressants in the acute and maintenance treatment of major depressive disorder: a review of registration trials. Expert Opinion on Pharmacotherapy, 10(18), 3061-3075. https://doi.org/10.1517/14656560903448837
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 17 of 22
It’s worth knowing that augmentation with bupropion, actually reduces SSRI side effects, it helps cancel out sexual side effects, may improve concentration a bit. But study after study has not shown better depression results by combining or adding bupropion to an SSRI. In the same vein, adding mirtazapine may improve sleep but does not improve refractory depression. So be aware that the atypical antipsychotics are more likely to be useful as augmentation agents.
References:
- Safarinejad, M. R. (2011). Reversal of SSRI-induced female sexual dysfunction by adjunctive bupropion in menstruating women: a double-blind, placebo-controlled and randomized study. Journal of Psychopharmacology, 25(3), 370-378. https://doi.org/10.1177/0269881109351966
- Alam, A., Voronovich, Z., & Carley, J. A. (2013). A Review of Therapeutic Uses of Mirtazapine in Psychiatric and Medical Conditions. The Primary Care Companion for CNS Disorders, 15(5), PCC.13r01525. https://doi.org/10.4088/PCC.13r01525
Slide 18 of 22
Dose recommendations are all modest doses and you should be seeing results in two weeks and four weeks should be an adequate trial of an adjunct agent before you adjust the dose or decide that it’s problematic.
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 19 of 22
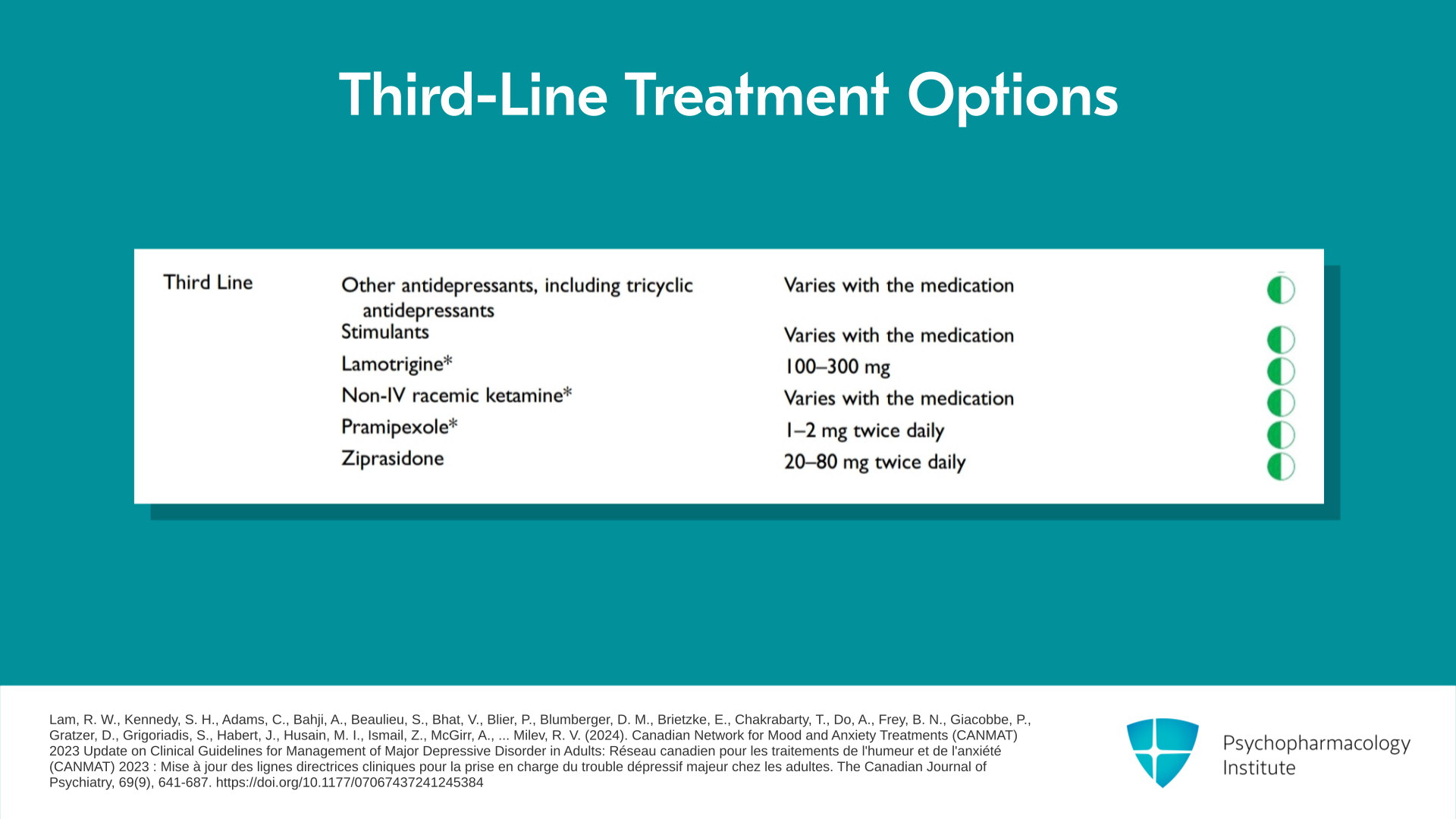
There are third-line recommendations for adjunct agents. Lamotrigine, Lamictal apart from the initial rash is very well tolerated and many clinicians and patients swear by it. But the evidence that it’s actually useful is very thin. Stimulants have a role and they are extremely helpful in improving functioning because many people with depression are left with residual low energy, poor concentration. And stimulants do help with functioning but they do not help with the person actually subjectively feeling better.
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Slide 20 of 22
A couple of cautionary notes. There’s a great interest in psychedelics but this is all investigational and we do not recommend microdosing or any other approach with psychedelics. And finally, if you want to get well with your depression, cannabis gets in the way and it is not “medical cannabis” or anything like that. Cannabis is not helpful and is probably harmful in the treatment of depression.
References:
- Lam, R. W., Kennedy, S. H., Adams, C., Bahji, A., Beaulieu, S., Bhat, V., Blier, P., Blumberger, D. M., Brietzke, E., Chakrabarty, T., Do, A., Frey, B. N., Giacobbe, P., Gratzer, D., Grigoriadis, S., Habert, J., Husain, M. I., Ismail, Z., McGirr, A., … Milev, R. V. (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry, 69(9), 641-687. https://doi.org/10.1177/07067437241245384
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 21 of 22
In summary, what are the key points? First of all, when choosing treatments, try several first-line treatments before going to second-line treatments. And a simple way to do this is to show the table of treatments to the patient. We go through the table together, and that way engage the patient to collaboratively review and choose treatments.
Slide 22 of 22
A second key point is that achieve at least a moderate dose of the medication and you don’t have to maximize it before you consider moving to another strategy. If the person is tolerating it and wants to maximize it, then that’s very reasonable to go. And the third key point is about augmentation agents. Lower doses are better. Start with aripiprazole at either 1 or 2 mg for two weeks and if they’re showing some benefit, hang in there for another two weeks. If they aren’t showing benefit either at two weeks or four weeks, you can consider another two-week trial at either 4 or 5 mg.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
