
Slides and Transcript
Slide 1 of 12
Colleagues, let's continue our discussion now about the long-term treatment of depression in later life with a more specific focus on maintenance treatments where the goal is to prevent relapse and recurrence.
Slide 2 of 12
Sometimes, we use the word relapse in connection with continuation therapy to ensure that the initial remission is stable. Typically, continuation therapy lasts about six months beyond the achievement of remission. And then at that point, we talk about longer-term maintenance therapy typically for one or two or even three years. The goal of maintenance treatment then is to prevent recurrence.
References:
- Reynolds, C. F. (2017). Evidence-Based Treatment and Prevention of Major Depressive Episodes in Later Life. In Halter, J. B., Ouslander, J. G., Studenski, S., High, K. P., Asthana, S., Supiano, M. A., Ritchie C. (Eds.), Hazzard's geriatric medicine and gerontology (7th ed., pp. 1071–1088). essay, McGraw-Hill Education Medical.

Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 12
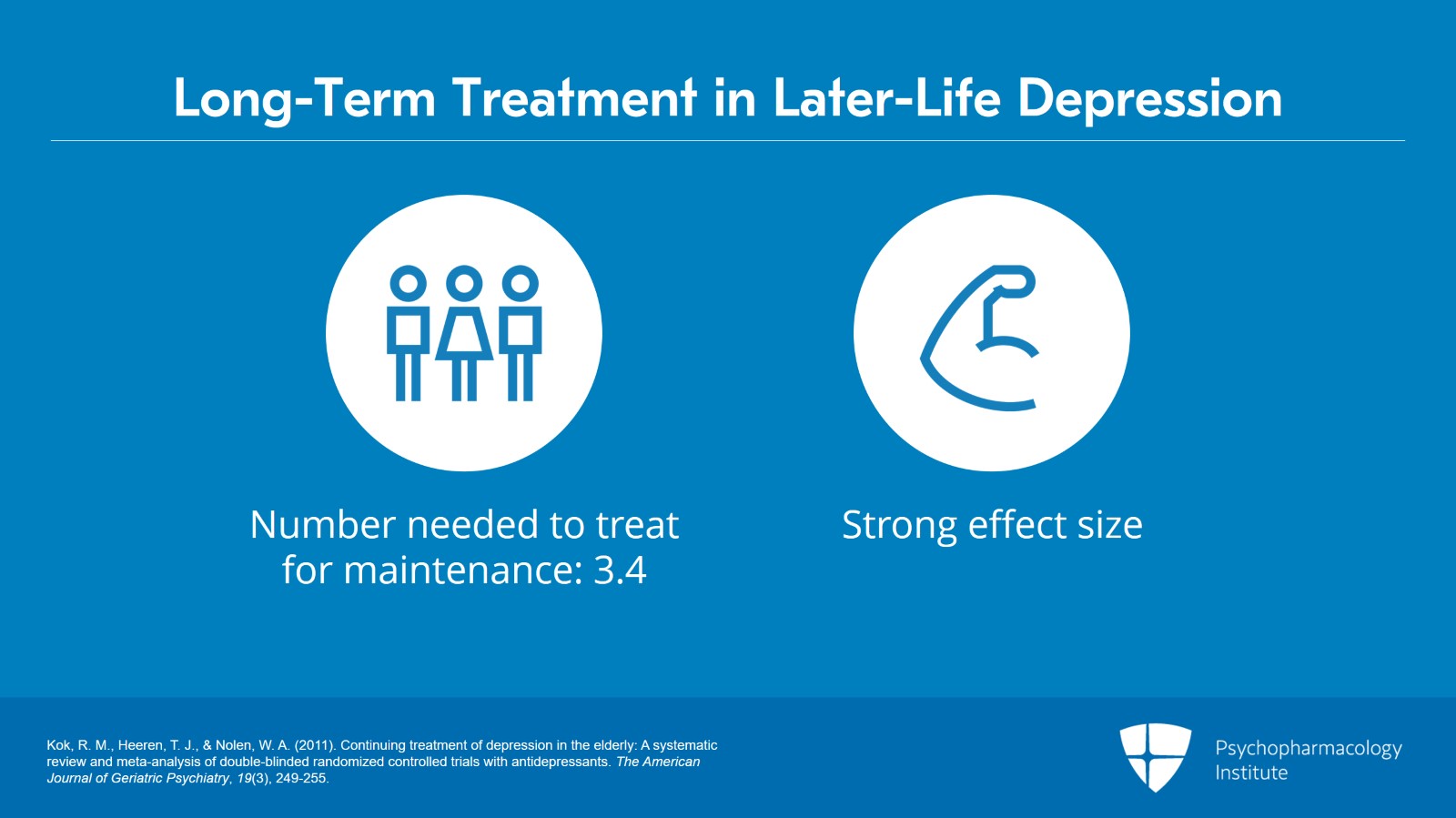
I'd like to draw, to introduce this part of our discussion on a systematic review and meta-analysis that was conducted by my colleague, Rob Kok. What we have said in essence to boil it down is that in the randomized placebo-controlled trials of maintenance pharmacotherapy in older depressed patients, the number needed to treat on average is 3.4. This is a moderately strong effect size. It means we need to treat three to four patients with maintenance pharmacotherapy to prevent recurrence for everyone that we would see with a pill placebo. Now, the number needed to treat in maintenance is considerably better than the number needed to treat as has been previously documented in earlier or acute phases of pharmacotherapy.
References:
- Kok, R. M., Heeren, T. J., & Nolen, W. A. (2011). Continuing treatment of depression in the elderly: A systematic review and meta-analysis of double-blinded randomized controlled trials with antidepressants. The American Journal of Geriatric Psychiatry, 19(3), 249-255.
Slide 4 of 12
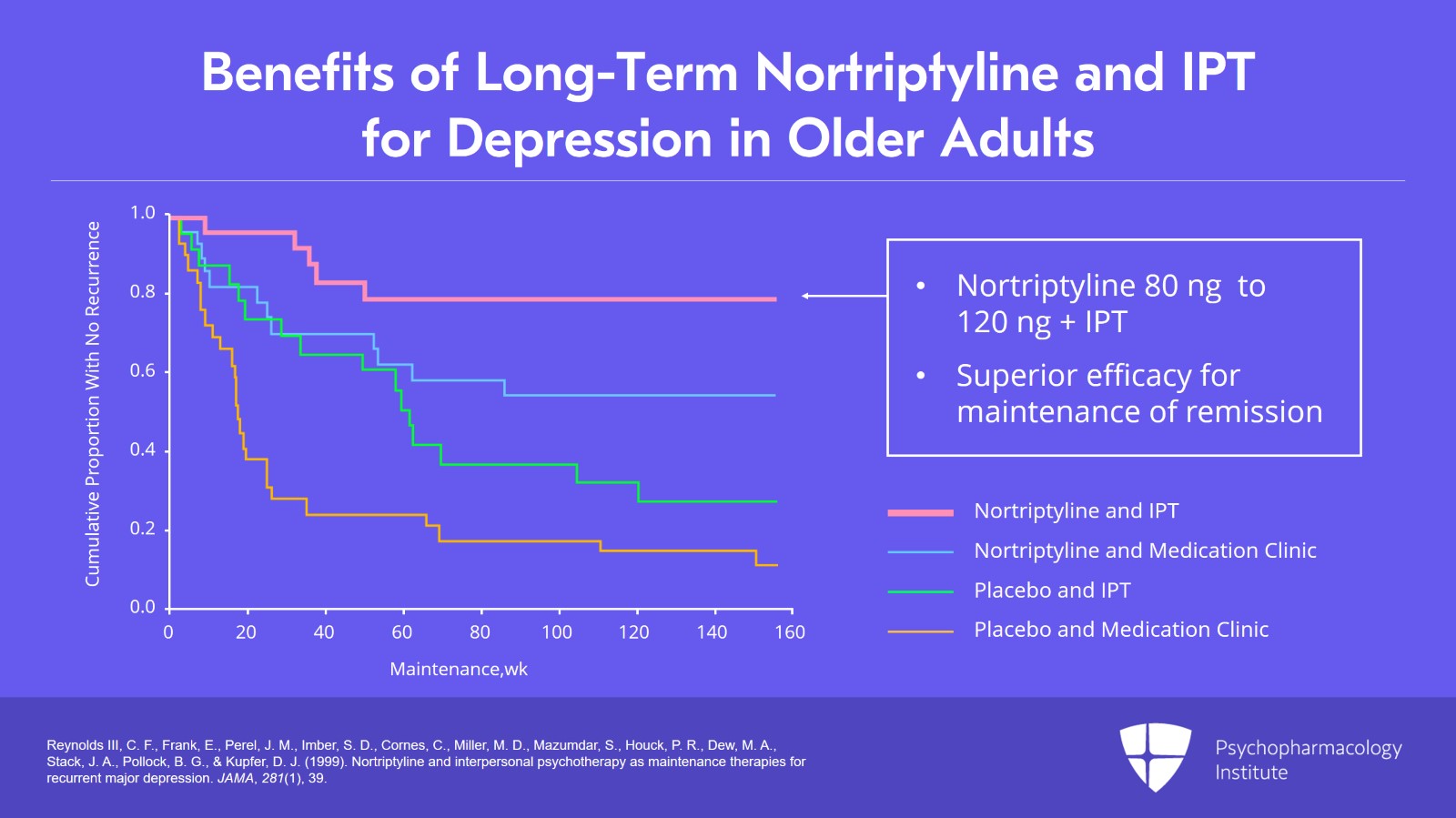
You'll see several figures here in this part of our talk and again this is from my laboratory and was the first of several maintenance trials that my group have performed over the past 20 years. The first slide shows the benefits of long-term nortriptyline and interpersonal psychotherapy for depression in older adults. These were young old patients with a mean age of 68 but with highly recurrent disease. The combination of nortriptyline at a steady state dose of 80 to 120 ng together with once monthly maintenance IPT showed a trend worthy superiority to drug alone in the maintenance of remission.
References:
- Reynolds III, C. F., Frank, E., Perel, J. M., Imber, S. D., Cornes, C., Miller, M. D., Mazumdar, S., Houck, P. R., Dew, M. A., Stack, J. A., Pollock, B. G., & Kupfer, D. J. (1999). Nortriptyline and interpersonal psychotherapy as maintenance therapies for recurrent major depression. JAMA, 281(1), 39.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 12
The second trial I'd like to draw your attention to colleagues again focusing on the benefits of long-term antidepressant pharmacotherapy is a trial that involved the use of maintenance paroxetine typically in doses of 20 to 40 mg a day together with once monthly maintenance IPT. This was a trial that my colleagues and I published in the New England Journal of Medicine back in 2006. And what we found in this study that paroxetine was superior to pill placebo over a two-year period in preventing recurrence.
References:
- Reynolds, C. F., 3rd, Dew, M. A., Pollock, B. G., Mulsant, B. H., Frank, E., Miller, M. D., Houck, P. R., Mazumdar, S., Butters, M. A., Stack, J. A., Schlernitzauer, M. A., Whyte, E. M., Gildengers, A., Karp, J., Lenze, E., Szanto, K., Bensasi, S., & Kupfer, D. J. (2006). Maintenance treatment of major depression in old age. The New England Journal of Medicine, 354(11), 1130–1138.

Slide 6 of 12
Of particular importance though and I think of great interest to colleagues who enjoy working in the interphase between Psychiatry and Primary Care Medicine, we examined the extent of concurrent medical burden, comorbidity, polymorbidity as a potential moderator of long-term treatment response. And what we found and reported in the New England Journal study was that these older patients, many of whom had considerable degrees of medical polymorbidity had a more brittle or fragile long-term response. They were more likely to suffer recurrence despite being on paroxetine. Another way of saying this is that concurrent medical burden, polymorbidity influenced or moderated the long-term strength of response to paroxetine.
References:
- Reynolds, C. F., 3rd, Dew, M. A., Pollock, B. G., Mulsant, B. H., Frank, E., Miller, M. D., Houck, P. R., Mazumdar, S., Butters, M. A., Stack, J. A., Schlernitzauer, M. A., Whyte, E. M., Gildengers, A., Karp, J., Lenze, E., Szanto, K., Bensasi, S., & Kupfer, D. J. (2006). Maintenance treatment of major depression in old age. The New England Journal of Medicine, 354(11), 1130–1138.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 12
The final study that I would like to mention in this section of our time together has to do with the question of cognitive impairment in older adults with depression and whether or not there is a place for the adjunctive use of an acetylcholinesterase inhibitor, donepezil, in the long-term maintenance treatment of such patients. This was the third maintenance trial that my colleagues and I performed again with NIMH support. This particular trial was published in the Archives of General Psychiatry back in 2011. Essentially, what we did in this study was to combine maintenance pharmacotherapy, antidepressant pharmacotherapy with donepezil generally in the doses of 5 to 10 mg in a randomized placebo-controlled trial. There were several interesting observations that emerged from this. Patients randomly assigned to antidepressant pharmacotherapy with donepezil as compared to patients randomly assigned to antidepressant pharmacotherapy with pill placebo, those on combination therapy indeed showed superior performance on cognitive instrumental activities of daily living at the point of one-year follow-up. It did make a difference at one year. By two years, however, the difference in cognitive instrumental activities of daily living was no longer statistically significant.
References:
- Reynolds, C. F., Butters, M. A., Lopez, O., Pollock, B. G., Dew, M. A., Mulsant, B. H., Lenze, E. J., Holm, M., Rogers, J. C., Mazumdar, S., Houck, P. R., Begley, A., Anderson, S., Karp, J. F., Miller, M. D., Whyte, E. M., Stack, J., Gildengers, A., Szanto, K., … DeKosky, S. T. (2011). Maintenance treatment of depression in old age. Archives of General Psychiatry, 68(1), 51.

Slide 8 of 12
The other observation that we made, and I would emphasize that this was a post hoc exploratory observation, was that amongst participants who entered the trial with a diagnosis not only of major depression but also mild cognitive impairment, the use of donepezil was associated with a statistically significant reduction in the transition from mild cognitive impairment to Alzheimer’s. We found specifically that patients randomly assigned to donepezil showed a 10% chance of transitioning from mild cognitive impairment to frank dementia as confirmed by Dr. Lopez while those randomly assigned to pill placebo had a 33% chance of transition. The downside of using donepezil, however, was a greater incidence of relapsing major depression. In other words, exposure to donepezil was also associated with a greater risk of recurrent major depression during the maintenance period.
References:
- Reynolds, C. F., Butters, M. A., Lopez, O., Pollock, B. G., Dew, M. A., Mulsant, B. H., Lenze, E. J., Holm, M., Rogers, J. C., Mazumdar, S., Houck, P. R., Begley, A., Anderson, S., Karp, J. F., Miller, M. D., Whyte, E. M., Stack, J., Gildengers, A., Szanto, K., … DeKosky, S. T. (2011). Maintenance treatment of depression in old age. Archives of General Psychiatry, 68(1), 51.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 9 of 12
The other point that I would like to emphasize before we close out this section of our time together has to do with the effects of long-term treatment on suicide risk and mortality risk. With respect to suicide risk, I'd like to cite the PROSPECT study, Prevention of Suicide in Primary Care Elderly, A Collaborative Trial. This is a multisite study that compared evidence-based depression care management in primary care settings with care as usual. We published an observation in JAMA back in 2004 that patients who were in practices randomized to depression care management, experienced a significantly faster and greater rate in reductions of suicidal ideation as compared with usual care practices. Then with respect to the issue of mortality risk over the long term, I'd like to mention a long-term follow-up of patients who had been in the PROSPECT study and who as a result of that had received at least two years of maintenance treatment using medication and to a considerable extent counseling with interpersonal psychotherapy. At nine-year follow-up, mortality risk was reduced by 24% amongst patients who had been in practices randomly assigned to evidence-based depression care management.
References:
- Bruce, M. L., Ten Have, T. R., Reynolds III, C. F., Katz, I. I., Schulberg, H. C., Mulsant, B. H., Brown, G. K., McAvay, G. J., Pearson, J. L., & Alexopoulos, G. S. (2004). Reducing suicidal ideation and depressive symptoms in depressed older primary care patients. JAMA, 291(9), 1081.
- Gallo, J. J., Morales, K. H., Bogner, H. R., Raue, P. J., Zee, J., Bruce, M. L., & Reynolds, C. F. (2013). Long term effect of depression care management on mortality in older adults: Follow-up of cluster randomized clinical trial in primary care. BMJ, 346, f2570.
Slide 10 of 12
So to summarize the key points here, remember depression is frequently a relapsing recurrent illness. Maintenance pharmacotherapy in older adults substantially reduces the risk for relapse and recurrence in studies lasting as long as two and three years. Secondly, the efficacy of maintenance pharmacotherapy is influenced or moderated by the extent of medical comorbidity.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 11 of 12
Patients with general medical comorbidity are more likely to have a brittle long-term response and to be liable to recurrence. Finally, evidence-based care for older primary care patients with major depression may lead to substantial reductions in risk for mortality over follow-up periods as long as eight to nine years. Thank you.
Slide 12 of 12

Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
