
Slides and Transcript
Slide 1 of 11
So we've talked a lot about psychopharmacologic treatments for PMS and PMDD. What about oral contraceptives? If PMS and PMDD are symptoms that occur only in the premenstrual period and have something to do with normal hormonal fluctuation, might it be useful to treat women with an oral contraceptive which evens out the hormonal fluctuation that women tend to experience across the menstrual cycle? Well, the short answer is yes. SSRIs we know are effective and they actually have lower risks overall than hormonal treatments so they should always be tried first
Slide 2 of 11
But for women who don't respond to SSRIs or for women who need hormonal contraception anyway, oral contraceptive pills can be another avenue to treatment. There's considerable evidence that if we suppress ovulation with an oral contraceptive pill, we can help the symptoms of women who have PMS or PMDD.
References:
- Schmidt, P. J., Nieman, L. K., Danaceau, M. A., Adams, L. F., & Rubinow, D. R. (1998). Differential behavioral effects of gonadal steroids in women with and in those without premenstrual syndrome. New England Journal of Medicine, 338(4), 209-216.

Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 11
Paradoxically, however, some women actually have adverse mood responses to hormonal contraceptives while other women benefit from them. So we don't actually know with any individual woman's case whether the oral contraceptive will help her. The evidence, however, to support oral contraceptive pills for PMDD is very strong and in fact is much stronger than that to support their use in PME, premenstrual exacerbation of an existing mood disorder. In PME, there are very few studies and the one well-designed trial actually showed no benefit. Side effects to oral contraceptives can include bloating and weight gain but for the most part, oral contraceptive pills are well tolerated by many patients. There are very few contraindications to the use of oral contraceptives in healthy young women. And delaying start while waiting an appointment with a gynecologist may actually deter some users.
References:
- Yonkers, K. A., Brown, C., Pearlstein, T. B., Foegh, M., Sampson-Landers, C., & Rapkin, A. (2005). Efficacy of a new low-dose oral contraceptive with drospirenone in premenstrual dysphoric disorder. Obstetrics & Gynecology, 106(3), 492-501.

Slide 4 of 11
For women with PMDD, there is particularly good evidence for oral contraceptives that contain the novel progestin called drospirenone. And the response rates for mood symptoms being improved for women who were on these medications were good and there have been several studies showing a response to these oral contraceptive pills. It's not entirely clear whether the good response to these medications comes about because of that novel progestin or comes about because these medications actually have a shorter placebo week than other oral contraceptives. Most oral contraceptive pills have a week of placebo pills towards the end. And shortening or eliminating that placebo week reduces hormonal fluctuation so that may be why they seem to be more effective.
References:
- Yonkers, K. A., Brown, C., Pearlstein, T. B., Foegh, M., Sampson-Landers, C., & Rapkin, A. (2005). Efficacy of a new low-dose oral contraceptive with drospirenone in premenstrual dysphoric disorder. Obstetrics & Gynecology, 106(3), 492-501.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 11
In fact, shortening or eliminating the placebo week will reduce hormonal fluctuation with any pill you take. So another good policy is to use any oral contraceptive continuously. So have the patient skip the placebo week and take only active pills.
References:
- Yonkers, K. A., Brown, C., Pearlstein, T. B., Foegh, M., Sampson-Landers, C., & Rapkin, A. (2005). Efficacy of a new low-dose oral contraceptive with drospirenone in premenstrual dysphoric disorder. Obstetrics & Gynecology, 106(3), 492-501.

Slide 6 of 11
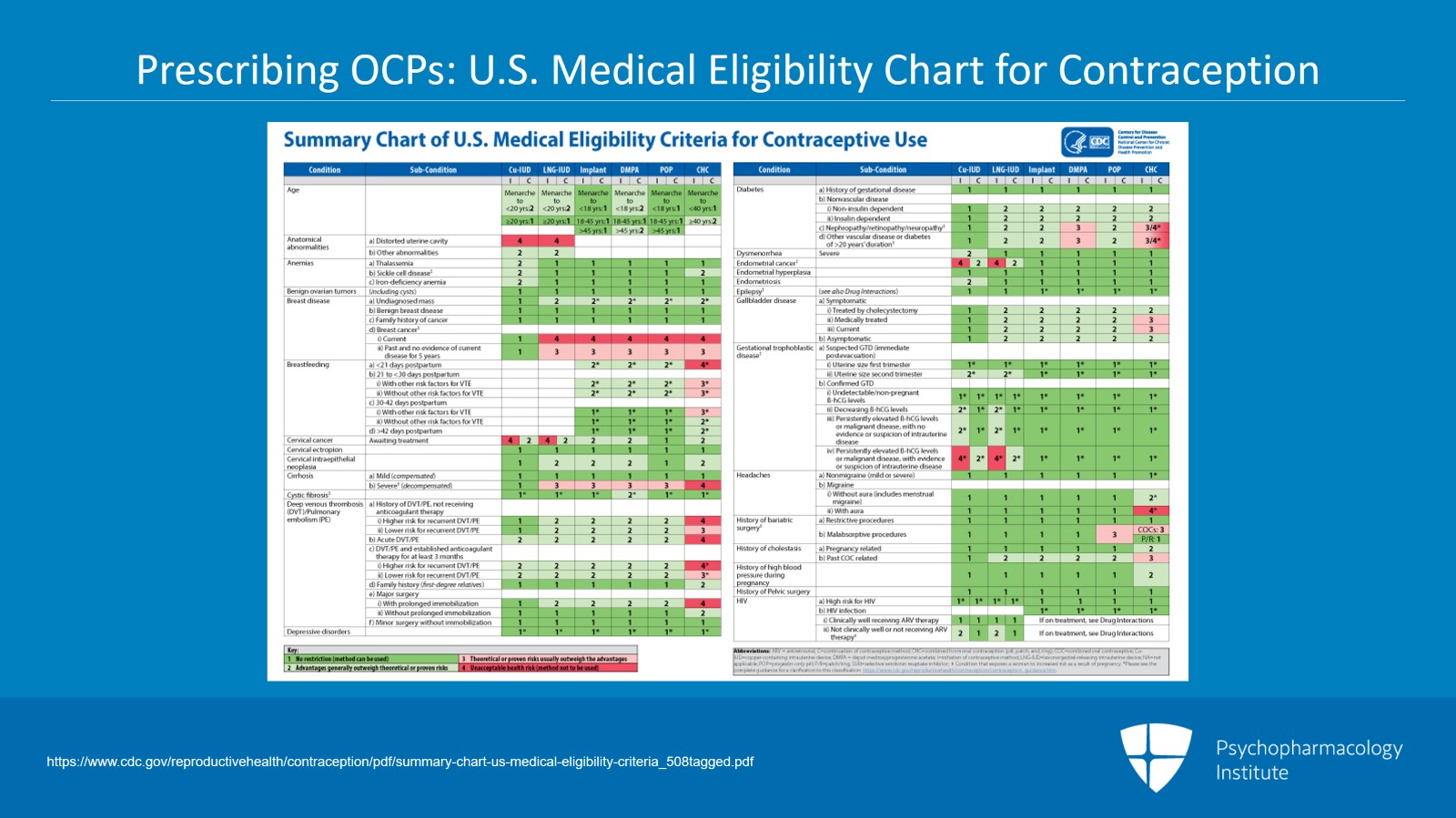
There's a US Medical Eligibility Chart for contraception that can walk you through the few things that are contraindications to starting an oral contraceptive and can help you become at ease with prescribing these medications yourself.
References:
- https://www.cdc.gov/reproductivehealth/contraception/pdf/summary-chart-us-medical-eligibility-criteria_508tagged.pdf
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 11
So the reason oral contraceptives may work is because they suppress ovulation and suppress that hormonal fluctuation by giving a steady state level of hormones across the menstrual cycle. In theory, of course, that means that suppressing ovulation by other means may also help women who suffer from luteal phase mood symptoms. Other methods of suppressing ovulation include GnRH agonist such as leuprolide, chemical oophorectomy or surgical oophorectomy. These methods may seem extreme and shouldn't be tried before the more benign approaches of SSRIs and OCPs. However, there are many trials showing the effectiveness of GnRH agonists for severe PMDD. There is no evidence, however, that they help with PME and some trials have shown no effect. So what about oophorectomy? What about moving to actual surgery to help women whose premenstrual symptoms are severe? What the evidence shows is that it is effective for those women who benefited from a trial with a GnRH agonist. So if you've undertaken a GnRH trial and the patient has benefited, that may be an indication that that woman would also benefit from an oophorectomy if she wants a permanent approach to ending her premenstrual symptoms. Oophorectomy, however, is untested in women who have PME. It's clear that not all women who undergo these more radical methods of ovulation suppression such as oophorectomy will actually benefit. One study showed that early oophorectomy measured in the general population is actually associated with increased symptoms of anxiety and depression.
References:
- Pinna, G. (2018). Biomarkers for PTSD at the interface of the endocannabinoid and neurosteroid axis. Front Neurosci 12: 482.
- Wyatt, K. M., Dimmock, P. W., Ismail, K. M., Jones, P. W., & O'Brien, P. S. (2004). The effectiveness of GnRHa with and without ‘add‐back’therapy in treating premenstrual syndrome: a meta analysis. BJOG: An International Journal of Obstetrics & Gynaecology, 111(6), 585-593.
- Rocca, W. A., Grossardt, B. R., Geda, Y. E., Gostout, B. S., Bower, J. H., Maraganore, D. M., … & Melton III, L. J. (2008). Long-term risk of depressive and anxiety symptoms after early bilateral oophorectomy. Menopause, 15(6), 1050-1059.

Slide 8 of 11
So it's something to be very careful about and we can see from this evidence that making that distinction between PMDD and PME is actually crucially important because some of our treatments of ovulation suppression do not seem to be at all effective in women with PME and it would be a travesty to have somebody undergo one of these more radical methods if it wasn't actually going to help her symptoms.
References:
- Rocca, W. A., Grossardt, B. R., Geda, Y. E., Gostout, B. S., Bower, J. H., Maraganore, D. M., … & Melton III, L. J. (2008). Long-term risk of depressive and anxiety symptoms after early bilateral oophorectomy. Menopause, 15(6), 1050-1059.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 9 of 11
So key points for this section. Women who don't respond to SSRIs and/or those who need hormonal contraception anyway may benefit from oral contraceptive pills. Oral contraceptive pills may help mood because they suppress ovulation and/or because the type of progesterone used is particularly helpful in combating symptoms of PMDD. You can use any oral contraceptive pill continuously eliminating the placebo week and thereby eliminating hormonal fluctuations and that can be a good choice for women. Although there are certain pills that are marketed for continuous use, you can actually use that approach with any pill.
Slide 10 of 11
Psychiatrists can and should learn to prescribe oral contraceptive pills. It's not difficult. There's a US Medical Eligibility Chart that can help. And often the waiting period to see another doctor to prescribe the pill may deter some patients from starting them. Other methods of ovulation suppression can also be effective in women with PMDD but they're indicated only in severe cases. Importantly, they may help women with PMDD but are either ineffective or untested in women who just have premenstrual exacerbation of another mood disorder.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 11 of 11

