
Slides and Transcript
Slide 1 of 18
The next part of the assessment for catatonia also brings us into treatment, this is a little bit unique, and that is the lorazepam challenge test. Again, this is an area where we have very little evidence base. So I’m going to give you a guide to how we do a lorazepam challenge test, but it’s important to recognize that there are different approaches, and these are not universally agreed upon.
Slide 2 of 18
One thing that has been studied is the dose for the lorazepam challenge, and what we know from the study is that a higher dose like 4 mg conveys no additional benefit over a standard dose of 2 mg. It hasn’t been studied whether 1 mg would be as effective as 2 mg, but in general but we give 2 mg in almost all cases because of the likelihood of getting an equivocal response at lower doses. If you don’t have lorazepam available, diazepam would be the next best option.
References:
- Suchandra, H. H., Reddi, V. S. K., Aandi Subramaniyam, B., & Muliyala, K. P. (2021). Revisiting lorazepam challenge test: Clinical response with dose variations and utility for catatonia in a psychiatric emergency setting. The Australian and New Zealand Journal of Psychiatry, 55(10), 993-1004. https://doi.org/10.1177/0004867420968915
- Gunther, M., Luccarelli, J., & Beach, S. (2025). Revisiting the lorazepam challenge: An algorithm for clinical-decision making. General Hospital Psychiatry, 93, 86–88. https://doi.org/10.1016/j.genhosppsych.2025.01.016
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 18
The situations in which I won’t use 2 mg, and I’ll use a lower dose are in pediatric patients, in very, very frail elderly patients. So in a healthy 80-year-old, I would still give 2 mg, but if I had somebody who is very frail, then I would think about giving a lower dose. And those who are at risk for respiratory compromise, I might also give a lower dose.
References:
- Suchandra, H. H., Reddi, V. S. K., Aandi Subramaniyam, B., & Muliyala, K. P. (2021). Revisiting lorazepam challenge test: Clinical response with dose variations and utility for catatonia in a psychiatric emergency setting. The Australian and New Zealand Journal of Psychiatry, 55(10), 993-1004. https://doi.org/10.1177/0004867420968915
- Gunther, M., Luccarelli, J., & Beach, S. (2025). Revisiting the lorazepam challenge: An algorithm for clinical-decision making. General Hospital Psychiatry, 93, 86–88. https://doi.org/10.1016/j.genhosppsych.2025.01.016
- Luccarelli, J., McCoy, T. H., Jr., York, T., Baldwin, I., Fricchione, G., Fuchs, C., & Smith, J. R. (2024). The effectiveness of the lorazepam challenge test in pediatric catatonia: A multisite retrospective cohort study. Schizophrenia Research, 270, 410-415. https://doi.org/10.1016/j.schres.2024.07.004
Slide 4 of 18
The lorazepam challenge is ideally performed using intravenous lorazepam. You can do it using oral lorazepam if you don’t have access, but you’re again more likely to get an equivocal response. For a one-time dose if I didn’t have intravenous lorazepam, I might go with intramuscular lorazepam for that challenge test though I won’t give somebody ongoing doses of intramuscular lorazepam if they’re catatonic for reasons that I’ll talk about later. It’s important to keep in mind that patients with catatonia are thought to be less susceptible to the sedative effects of benzodiazepines, but if they do get sedated that doesn’t necessarily mean that they don’t have catatonia.
References:
- Suchandra, H. H., Reddi, V. S. K., Aandi Subramaniyam, B., & Muliyala, K. P. (2021). Revisiting lorazepam challenge test: Clinical response with dose variations and utility for catatonia in a psychiatric emergency setting. The Australian and New Zealand Journal of Psychiatry, 55(10), 993-1004. https://doi.org/10.1177/0004867420968915
- Gunther, M., Luccarelli, J., & Beach, S. (2025). Revisiting the lorazepam challenge: An algorithm for clinical-decision making. General Hospital Psychiatry, 93, 86–88. https://doi.org/10.1016/j.genhosppsych.2025.01.016
- Luccarelli, J., McCoy, T. H., Jr., York, T., Baldwin, I., Fricchione, G., Fuchs, C., & Smith, J. R. (2024). The effectiveness of the lorazepam challenge test in pediatric catatonia: A multisite retrospective cohort study. Schizophrenia Research, 270, 410-415. https://doi.org/10.1016/j.schres.2024.07.004
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 18
The response to a lorazepam challenge is variable. There have actually been some authors who recommend only giving lorazepam challenge test five minutes to work, and then repeating it if there’s no response. We recommend waiting a longer period of time in between doses. Some patients will respond within seconds to minutes. That’s kind of that Lazarus effect, but that tends to be the minority of patients. Most patients will respond within 30 minutes, but sometimes patients can take up to 2 to 3 hours to respond. So I generally wait between 1 to 2 hours before I’m going to repeat the lorazepam challenge, or make a final decision if a patient hasn’t responded. With regard to the lorazepam challenge, it’s important to recognize too that it has been successfully used in pediatric populations in addition to adult populations.
References:
- Suchandra, H. H., Reddi, V. S. K., Aandi Subramaniyam, B., & Muliyala, K. P. (2021). Revisiting lorazepam challenge test: Clinical response with dose variations and utility for catatonia in a psychiatric emergency setting. The Australian and New Zealand Journal of Psychiatry, 55(10), 993-1004. https://doi.org/10.1177/0004867420968915
- Gunther, M., Luccarelli, J., & Beach, S. (2025). Revisiting the lorazepam challenge: An algorithm for clinical-decision making. General Hospital Psychiatry, 93, 86–88. https://doi.org/10.1016/j.genhosppsych.2025.01.016
- Luccarelli, J., McCoy, T. H., Jr., York, T., Baldwin, I., Fricchione, G., Fuchs, C., & Smith, J. R. (2024). The effectiveness of the lorazepam challenge test in pediatric catatonia: A multisite retrospective cohort study. Schizophrenia Research, 270, 410-415. https://doi.org/10.1016/j.schres.2024.07.004
Slide 6 of 18
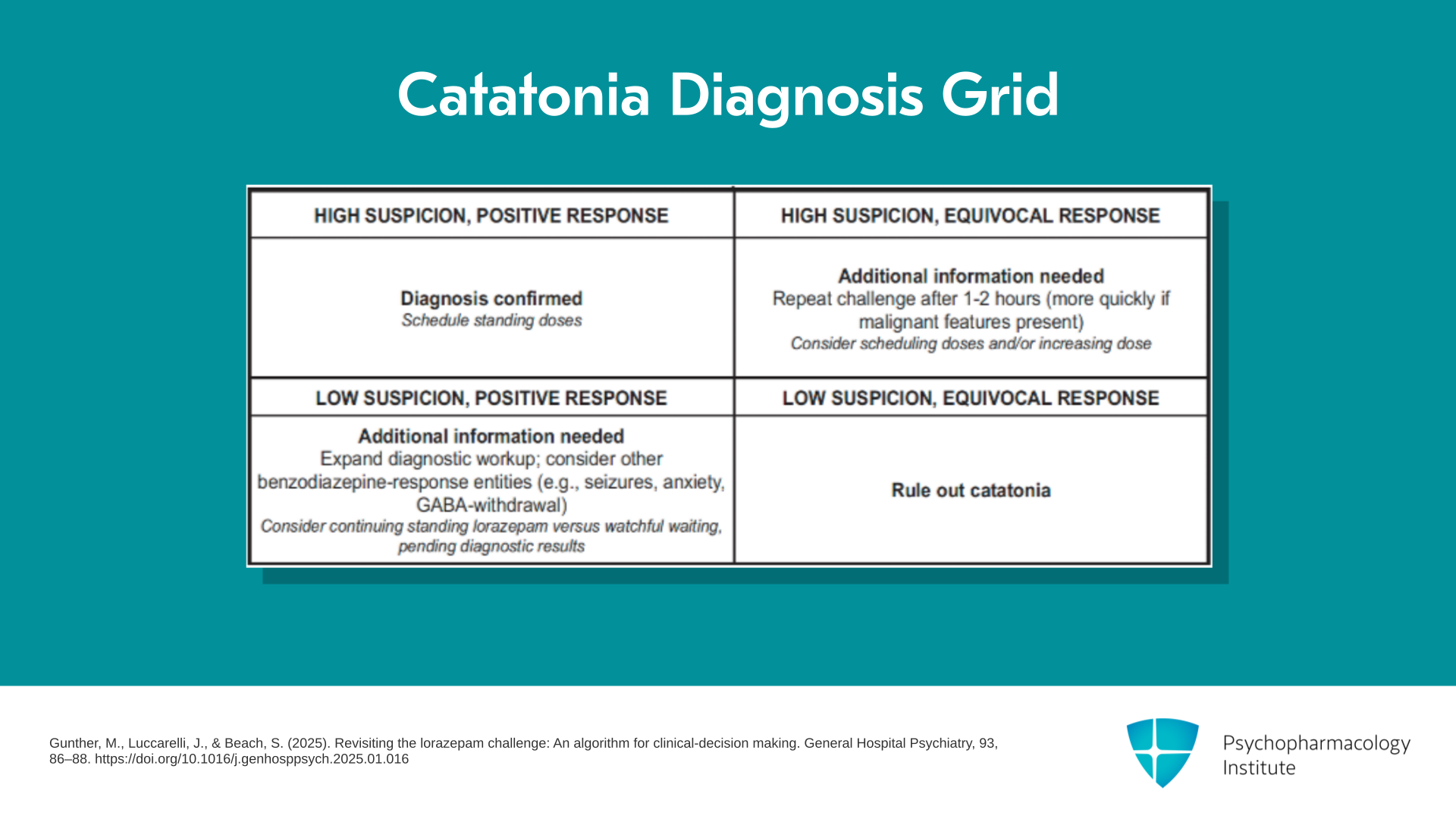
The way that we think about the lorazepam challenge test and the response to the lorazepam challenge is using a 2×2 grid, that’s based on your pretest probability and the response to the challenge.
References:
- Suchandra, H. H., Reddi, V. S. K., Aandi Subramaniyam, B., & Muliyala, K. P. (2021). Revisiting lorazepam challenge test: Clinical response with dose variations and utility for catatonia in a psychiatric emergency setting. The Australian and New Zealand Journal of Psychiatry, 55(10), 993-1004. https://doi.org/10.1177/0004867420968915
- Gunther, M., Luccarelli, J., & Beach, S. (2025). Revisiting the lorazepam challenge: An algorithm for clinical-decision making. General Hospital Psychiatry, 93, 86–88. https://doi.org/10.1016/j.genhosppsych.2025.01.016
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 18
The first thing to think about is what represents a positive response to the lorazepam challenge. Again, there’s not great agreement on this, and it’s never really been studied. What’s been traditionally recommended is that there needs to be a 50% reduction in the Bush-Francis score in order to qualify as a positive response. That’s really not based on any evidence. It’s just based on the fact that 50% reduction is often used as evidence of a positive response in other scales, like depression rating scales, for example. I would argue that that’s a pretty high threshold for a positive response, and I have definitely seen patients who demonstrate a meaningful change in symptomatology after getting a dose of lorazepam without actually improving their Bush-Francis score by 50%.
References:
- Suchandra, H. H., Reddi, V. S. K., Aandi Subramaniyam, B., & Muliyala, K. P. (2021). Revisiting lorazepam challenge test: Clinical response with dose variations and utility for catatonia in a psychiatric emergency setting. The Australian and New Zealand Journal of Psychiatry, 55(10), 993-1004. https://doi.org/10.1177/0004867420968915
- Gunther, M., Luccarelli, J., & Beach, S. (2025). Revisiting the lorazepam challenge: An algorithm for clinical-decision making. General Hospital Psychiatry, 93, 86–88. https://doi.org/10.1016/j.genhosppsych.2025.01.016
Slide 8 of 18
So I think about a positive response as involving either obvious changes in multiple symptom domains, that’s kind of the ideal situation, or sometimes a significant change in even one symptom domain. So if a patient was previously completely mute and now they’re speaking 5 to 10 words a minute after the lorazepam challenge test, even if all of their other symptoms remain unchanged, I would probably consider that to be a positive response because to me that’s a meaningful change in a key symptom. Partial responses in my mind are positive responses but again there’s no universal agreement.
References:
- Suchandra, H. H., Reddi, V. S. K., Aandi Subramaniyam, B., & Muliyala, K. P. (2021). Revisiting lorazepam challenge test: Clinical response with dose variations and utility for catatonia in a psychiatric emergency setting. The Australian and New Zealand Journal of Psychiatry, 55(10), 993-1004. https://doi.org/10.1177/0004867420968915
- Gunther, M., Luccarelli, J., & Beach, S. (2025). Revisiting the lorazepam challenge: An algorithm for clinical-decision making. General Hospital Psychiatry, 93, 86–88. https://doi.org/10.1016/j.genhosppsych.2025.01.016
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 9 of 18
For a negative response, I might consider that to be a patient who has no changes, or they have subtle changes that are really questionable in terms of their reproducibility or could be due to randomness. So for example, if I had somebody who I thought maybe had slightly less rigidity after the lorazepam challenge, but it was hard to tell and their other symptoms didn’t change, I probably would consider that a negative response. Again, I come back to the idea that sedation does not automatically indicate a negative response. Patients with catatonia do have a higher threshold for sedation but I’ve seen a lot of patients with catatonia who get a dose of lorazepam, they fall asleep and they wake up 30 minutes later and they actually look much better.
References:
- Suchandra, H. H., Reddi, V. S. K., Aandi Subramaniyam, B., & Muliyala, K. P. (2021). Revisiting lorazepam challenge test: Clinical response with dose variations and utility for catatonia in a psychiatric emergency setting. The Australian and New Zealand Journal of Psychiatry, 55(10), 993-1004. https://doi.org/10.1177/0004867420968915
- Gunther, M., Luccarelli, J., & Beach, S. (2025). Revisiting the lorazepam challenge: An algorithm for clinical-decision making. General Hospital Psychiatry, 93, 86–88. https://doi.org/10.1016/j.genhosppsych.2025.01.016
Slide 10 of 18
The other part of our algorithm is whether you started with high suspicion or low suspicion. Again, these are hard things to define and we don’t have great guidance into what low suspicion or high suspicion means, but a few things that I think about with regard to patients who I consider high suspicion for catatonia prior to the lorazepam challenge are the following: “Do they have a history of catatonia?” If yes, that may put them in the high suspicion category. “Do they have symptoms in multiple domains, meaning they have both motor symptoms and behavioral symptoms?” If so, that might put them in the high suspicion category for me.
References:
- Suchandra, H. H., Reddi, V. S. K., Aandi Subramaniyam, B., & Muliyala, K. P. (2021). Revisiting lorazepam challenge test: Clinical response with dose variations and utility for catatonia in a psychiatric emergency setting. The Australian and New Zealand Journal of Psychiatry, 55(10), 993-1004. https://doi.org/10.1177/0004867420968915
- Gunther, M., Luccarelli, J., & Beach, S. (2025). Revisiting the lorazepam challenge: An algorithm for clinical-decision making. General Hospital Psychiatry, 93, 86–88. https://doi.org/10.1016/j.genhosppsych.2025.01.016
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 11 of 18
Although we know that Bush-Francis score does not correlate to severity, if somebody has a very high score like above 20, that’s going to push them into the higher suspicion category for me. Whereas, somebody who has a very low score like below 7, for example, that might push them into the low suspicion category.
References:
- Suchandra, H. H., Reddi, V. S. K., Aandi Subramaniyam, B., & Muliyala, K. P. (2021). Revisiting lorazepam challenge test: Clinical response with dose variations and utility for catatonia in a psychiatric emergency setting. The Australian and New Zealand Journal of Psychiatry, 55(10), 993-1004. https://doi.org/10.1177/0004867420968915
- Gunther, M., Luccarelli, J., & Beach, S. (2025). Revisiting the lorazepam challenge: An algorithm for clinical-decision making. General Hospital Psychiatry, 93, 86–88. https://doi.org/10.1016/j.genhosppsych.2025.01.016
Slide 12 of 18
And then the final thing to consider is the likelihood of other diagnoses, other things that might look like catatonia but are not actually catatonia. We sometimes call those catatonia mimics, and we’ll talk more about them. If I have a high suspicion for a catatonia mimic, then that might make me have a lower suspicion for catatonia. And conversely, if I have a low suspicion for a catatonic mimic, that might make me have a high suspicion.
References:
- Suchandra, H. H., Reddi, V. S. K., Aandi Subramaniyam, B., & Muliyala, K. P. (2021). Revisiting lorazepam challenge test: Clinical response with dose variations and utility for catatonia in a psychiatric emergency setting. The Australian and New Zealand Journal of Psychiatry, 55(10), 993-1004. https://doi.org/10.1177/0004867420968915
- Gunther, M., Luccarelli, J., & Beach, S. (2025). Revisiting the lorazepam challenge: An algorithm for clinical-decision making. General Hospital Psychiatry, 93, 86–88. https://doi.org/10.1016/j.genhosppsych.2025.01.016
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 13 of 18
So we’ve got pretest high versus low suspicion, then posttest positive versus negative response, and that allows us to build a 2×2 grid in order to inform next steps. If you had a positive response in a case where you already had high suspicion, then you’ve essentially confirmed the diagnosis of catatonia and you can begin scheduling standing doses of benzodiazepines. Conversely, if you had a negative or equivocal response in a case that was low suspicion to begin with, then you’ve essentially ruled out catatonia, and you can move on to thinking about what else might be going on.
References:
- Gunther, M., Luccarelli, J., & Beach, S. (2025). Revisiting the lorazepam challenge: An algorithm for clinical-decision making. General Hospital Psychiatry, 93, 86–88. https://doi.org/10.1016/j.genhosppsych.2025.01.016
Slide 14 of 18
If you started with a low suspicion but you had a positive response to the lorazepam challenge, that’s an indication that you need additional information. In that case, I would expand my diagnostic workup and I would especially consider other entities that may be responsive to benzodiazepines, primarily anxiety, seizures or GABA withdrawal because all of those things are going to respond positively to a lorazepam challenge as well.
References:
- Gunther, M., Luccarelli, J., & Beach, S. (2025). Revisiting the lorazepam challenge: An algorithm for clinical-decision making. General Hospital Psychiatry, 93, 86–88. https://doi.org/10.1016/j.genhosppsych.2025.01.016
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 15 of 18
On the flip side, if you started with a high suspicion for catatonia but you had an equivocal or a negative response to the lorazepam challenge, that is again a situation where additional information is needed. It doesn’t rule out catatonia. In that case, I would probably repeat the challenge, again usually waiting one to two hours though I would move more quickly if any malignant features were present and I would consider scheduling doses or increasing the dose.
References:
- Gunther, M., Luccarelli, J., & Beach, S. (2025). Revisiting the lorazepam challenge: An algorithm for clinical-decision making. General Hospital Psychiatry, 93, 86–88. https://doi.org/10.1016/j.genhosppsych.2025.01.016
Slide 16 of 18
We know from a study that across the board 4 mg is not more effective than 2 mg, but you will undoubtedly encounter patients who don’t respond to 2 mg but do respond to 3 or 4 mg. So that instance, high suspicion for catatonia but initial equivocal response, might be a case where you would think about either repeating the challenge several times or increasing the dose of the challenge.
References:
- Suchandra, H. H., Reddi, V. S. K., Aandi Subramaniyam, B., & Muliyala, K. P. (2021). Revisiting lorazepam challenge test: Clinical response with dose variations and utility for catatonia in a psychiatric emergency setting. The Australian and New Zealand Journal of Psychiatry, 55(10), 993-1004. https://doi.org/10.1177/0004867420968915
- Gunther, M., Luccarelli, J., & Beach, S. (2025). Revisiting the lorazepam challenge: An algorithm for clinical-decision making. General Hospital Psychiatry, 93, 86–88. https://doi.org/10.1016/j.genhosppsych.2025.01.016
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 17 of 18
So to summarize, a few key points for this section: The lorazepam challenge test or LCT is a widely used approach to both confirming the diagnosis of catatonia and initiating early treatment. Response to the LCT should be evaluated on the basis of both pretest suspicion for catatonia as well as considering the entire clinical picture, and response to the challenge.
Slide 18 of 18
While a positive response to the LCT has traditionally been considered to be a 50% or greater reduction in symptoms, this threshold may be too strict and meaningful improvement in one or multiple symptom domains could be considered evidence of a positive response.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
