
Fluoxetine has activating properties that make it a good option for patients with retarded depression or atypical depression. However, we should avoid activation in patients with insomnia and agitation. There is something that makes fluoxetine unique: its long half-life, we will discuss the advantages and disadvantages of this in clinical practice. This long half-life allowed the development of a weekly capsule. The other important pharmacokinetic concept is that fluoxetine is a potent inhibitor of the CYP2D6.
Pharmacology and MOA

As other SSRIs, fluoxetine inhibits the serotonin transporter protein. In addition, it is also a weak norepinephrine reuptake inhibitor, this effect increases with higher doses. However, the clinical relevance of this norepinephrine effect is not clear. Fluoxetine is an antagonist at 5HT2C receptors, this has been proposed as a potential mechanism for its activating properties.
Clinical Uses
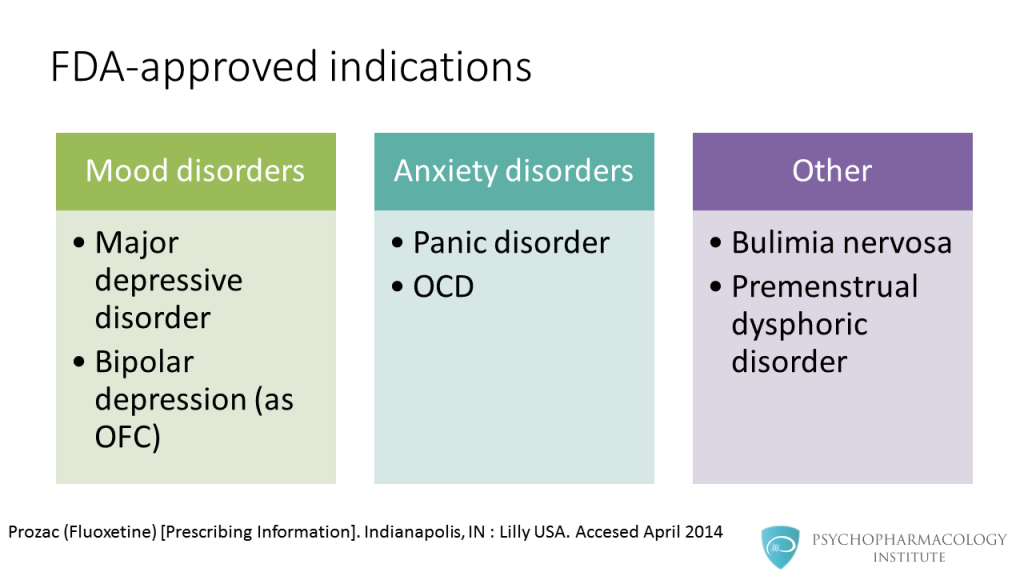
Fluoxetine is approved for the treatment of major depressive disorder and bipolar depression. In the case of bipolar depression, its use is approved in a combined olanzapine formulation, called olanzapine-fluoxetine combination, or OFC (Symbyax). It is also approved for anxiety disorders such as panic disorder and OCD. Other indications include bulimia nervosa and premenstrual dysphoric disorder. Fluoxetine is the only antidepressant approved for the treatment of bulimia.
Pharmacokinetics



Fluoxetine is a potent CYP2D6 inhibitor, the drug shares this feature with two other SSRIs: paroxetine and fluvoxamine. This opens the possibility of drug-drug interactions with CYP2D6 substrates. Norfluoxetine, its active metabolite is a moderate CYP3A4 inhibitor, but this is not clinically relevant.
Adverse effects

Regarding side effects, it has a similar profile to other members of the SSRI class. There is one distinctive side effect related to its clinical profile: the possibility of causing activation. This is seen as nervousness or insomnia, it is usually transient, appears usually at the beginning of therapy and then remits. This should be kept in mind when prescribing fluoxetine to depressed patients with anxiety.
Prescribing information


Fluoxetine is available in a number of formulations.
- Capsules of 10 mg, 20 mg and 40 mg
- 10 mg tablet
- Liquid formulation of 20 mg/5ml, this is available in 120 ml bottles
- Weekly capsule of 90 mg, this allows once weekly dosing
- Fluvoxamine Essentials: Mechanism of Action, Indications, Pharmacokinetics and Dosing
- Sertraline Essentials: Mechanism of Action, Indications, Pharmacokinetics and Dosing
- Citalopram and Escitalopram: A Summary of Key Differences and Similarities
- The Psychopharmacology of Paroxetine: An Illustrated Summary for Prescribers
Note: this video has been translated to Spanish “
Fluoxetina: farmacodinamia, indicaciones, efectos adversos, farmacocinética y posología
“
References
- Hindmarch, I., & Hashimoto, K. (2010). Cognition and depression: the effects of fluvoxamine, a sigma‐1 receptor agonist, reconsidered . Human Psychopharmacology: Clinical and Experimental, 25(3), 193-200.
- Schatzberg, Alan F., and Charles B. Nemeroff, eds. The American psychiatric publishing textbook of psychopharmacology . American Psychiatric Pub, 2009.
- Luvox CR (Fluvoxamine CR) [Prescribing Information]. Palo Alto, CA: Jazz Pharmaceuticals, Inc. Accessed May 2014.
- Serretti, A., & Mandelli, L. (2010). Antidepressants and body weight: a comprehensive review and meta-analysis . The Journal of clinical psychiatry,71(10), 1259-1272.
- Sadock, B J., V A. Sadock, and P Ruiz. Kaplan and Sadock’s Comprehensive Textbook of Psychiatry. 9th ed. Philadelphia: Lippincott Williams & Wilk
