
Slides and Transcript
Slide 1 of 24
I want to talk about what withdrawal effects are and misdiagnoses often made.
Slide 2 of 24
There is a long list of withdrawal symptoms. I list just a selected group here – dizziness, insomnia, impaired concentration, fatigue, headache, tremor, tachycardia, nightmares. There are mood symptoms, depressed mood, irritability, anxiety, panic attacks.
References:
- Fava, G. A., Gatti, A., Belaise, C., Guidi, J., & Offidani, E. (2015). Withdrawal symptoms after selective serotonin reuptake inhibitor discontinuation: A systematic review. Psychotherapy and Psychosomatics, 84(2), 72–81. https://doi.org/10.1159/000370338
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 24
We know that these are withdrawal symptoms and not just a return of people’s underlying condition because in studies in which people are given antidepressants without any underlying mental health conditions, so in studies involving people with pain syndromes or the menopause or even in healthy volunteers, people can show these psychological symptoms.
References:
- Fava, G. A., Gatti, A., Belaise, C., Guidi, J., & Offidani, E. (2015). Withdrawal symptoms after selective serotonin reuptake inhibitor discontinuation: A systematic review. Psychotherapy and Psychosomatics, 84(2), 72–81. https://doi.org/10.1159/000370338
- Gallagher, J. C., Strzinek, R. A., Cheng, R. F., Ausmanas, M. K., Astl, D., & Seljan, P. (2012). The effect of dose titration and dose tapering on the tolerability of desvenlafaxine in women with vasomotor symptoms associated with menopause. Journal of Women's Health, 21(2), 188–198. https://doi.org/10.1089/jwh.2011.2764
Slide 4 of 24
There are some quite distinctive sensory symptoms. I mentioned electric shock sensations in the head or in the limbs, but you can have burning skin, all sorts of neurological symptoms. There are gut symptoms, because there is a lot of serotonergic neurons in the gut. There’s also an increase in suicide attempts in the weeks after stopping an antidepressant, even in people who have not been suicidal before which has been attributed to withdrawal effects themselves and not just a relapse.
References:
- Fava, G. A., Gatti, A., Belaise, C., Guidi, J., & Offidani, E. (2015). Withdrawal symptoms after selective serotonin reuptake inhibitor discontinuation: A systematic review. Psychotherapy and Psychosomatics, 84(2), 72–81. https://doi.org/10.1159/000370338
- Valuck, R. J., Orton, H. D., & Libby, A. M. (2009). Antidepressant discontinuation and risk of suicide attempt: a retrospective, nested case-control study. The Journal of Clinical Psychiatry, 70(8), 1069–1077. https://doi.org/10.4088/JCP.08m04943
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 24
And another symptom which is often overlooked to the peril of patients is akathisia. Although this is recognized as a long-term effect of antipsychotic use, it is also a consequence of withdrawal from antidepressants and other psychiatric drugs, especially when done too quickly. These are the sickest patients I see in my practice. They are often pacing. They express a sense of terror. They describe feeling like their nervous system is on fire.
References:
- Fava, G. A., Gatti, A., Belaise, C., Guidi, J., & Offidani, E. (2015). Withdrawal symptoms after selective serotonin reuptake inhibitor discontinuation: A systematic review. Psychotherapy and Psychosomatics, 84(2), 72–81. https://doi.org/10.1159/000370338
- Henssler, J., Heinz, A., Brandt, L., & Bschor, T. (2019). Antidepressant withdrawal and rebound phenomena. Deutsches Ärzteblatt International, 116(20), 355-361. https://doi.org/10.3238/arztebl.2019.0355
Slide 6 of 24
And the word akathisia comes from the Greek meaning cannot keep still although in some people it’s much more of an inner experience rather than involving frank pacing. These people are so disturbed that there’s a high risk of suicide, because they do not get a break week after week, and sometimes this condition can last months and even years. Because it is not widely recognized by clinicians, it is often misdiagnosed when people turn up to the emergency department or to clinics as agitated depression, mania or even psychosis.
References:
- Fava, G. A., Gatti, A., Belaise, C., Guidi, J., & Offidani, E. (2015). Withdrawal symptoms after selective serotonin reuptake inhibitor discontinuation: A systematic review. Psychotherapy and Psychosomatics, 84(2), 72–81. https://doi.org/10.1159/000370338
- Valuck, R. J., Orton, H. D., & Libby, A. M. (2009). Antidepressant discontinuation and risk of suicide attempt: a retrospective, nested case-control study. The Journal of Clinical Psychiatry, 70(8), 1069–1077. https://doi.org/10.4088/JCP.08m04943
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 24
Another major issue is misdiagnosing antidepressant withdrawal as relapse. It’s reported to occur by patients often but not studied systematically. In our survey of more than 1000 people out of the almost 200,000 people on peer support websites, it was the main reason they gave for being there. It’s easy to see why this occurs because withdrawal symptoms can include anxiety, depressed mood, insomnia. And whilst guidelines have described these symptoms as mild and brief for a couple of decades, when someone with these symptoms that can be severe or long-lasting turns up to your clinic, it’s easy to flash on relapse rather than withdrawal.
References:
- Horowitz, M. A., & Taylor, D. (2022). Distinguishing relapse from antidepressant withdrawal: Clinical practice and antidepressant discontinuation studies. BJPsych Advances, 28(5), 297–311. https://doi.org/10.1192/bja.2021.62
Slide 8 of 24
There are a few clues to distinguish withdrawal from relapse. Withdrawal effects tend to be quicker in onset, often in a few days after reducing or stopping a drug, but they can also be delayed in onset by several weeks, probably because it takes downstream effects time to build up which can be very confusing for clinicians and for patients. There are specific symptoms in withdrawal. Things like dizziness, electric shock sensations are very distinctive of withdrawal.
References:
- Horowitz, M. A., & Taylor, D. (2022). Distinguishing relapse from antidepressant withdrawal: Clinical practice and antidepressant discontinuation studies. BJPsych Advances, 28(5), 297–311. https://doi.org/10.1192/bja.2021.62
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 9 of 24
But in fact the most common symptoms of withdrawal are psychological symptoms. And so sometimes patients will tell you the diagnosis. They will say, I have never felt like this before, or this is much more severe than my underlying condition. It’s very useful to know what people’s underlying symptoms were before starting medication to make a comparison. So for example, if you see a patient who went on medication because they were feeling low, they were lethargic, they were spending large amounts of time sleeping after their mother died and now a few years later, when they come off their antidepressants, they are anxious, can’t sleep, having panic attacks, it’s much more likely that they’ve developed quite common withdrawal effects rather than coincidentally at the moment they’ve stopped an antidepressant developed a new-onset panic disorder, although often clinicians that are unfamiliar with withdrawal effects will make that misdiagnosis.
References:
- Horowitz, M. A., & Taylor, D. (2022). Distinguishing relapse from antidepressant withdrawal: Clinical practice and antidepressant discontinuation studies. BJPsych Advances, 28(5), 297–311. https://doi.org/10.1192/bja.2021.62
Slide 10 of 24
The last point is that if antidepressants are restarted soon after withdrawal effects come on, often there’s quick resolution of symptoms, but if reinstatement is delayed for longer, results are much more unpredictable. And withdrawal effects can also be misdiagnosed as chronic fatigue syndrome, medically unexplained symptoms, functional neurological disorder or a wide range of psychiatric, gastroenterological, and neurological disorders, because their symptoms overlap with the diagnostic criteria of many of these conditions.
References:
- Horowitz, M. A., & Taylor, D. (2022). Distinguishing relapse from antidepressant withdrawal: Clinical practice and antidepressant discontinuation studies. BJPsych Advances, 28(5), 297–311. https://doi.org/10.1192/bja.2021.62
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 11 of 24
So how common, severe, and long-lasting are withdrawal symptoms? There was a high-profile study published on this topic in the Lancet Psychiatry at the end of 2024 by Henssler and colleagues, and it reported that withdrawal effects, if you subtract nocebo withdrawal effects, occur to only 1 in 6 people, and severe withdrawal only occurs to about 3% of people. And that was seen as a reassuring message that these withdrawal effects were not as common as some other systematic reviews had revealed. The problem with this study is that three-quarters of the studies captured by it were conducted by drug companies.
References:
- Henssler, J., Schmidt, Y., Schmidt, U., Schwarzer, G., Bschor, T., & Baethge, C. (2024). Incidence of antidepressant discontinuation symptoms: a systematic review and meta‑analysis. The Lancet Psychiatry. Advance online publication. https://doi.org/10.1016/S2215-0366(24)00133-0
Slide 12 of 24
These were 8-12-week studies. In these studies, withdrawal was mostly assessed by spontaneous reports, not systematically. In other words, patients had to go to the researchers, and tell them if they experienced any odd symptoms rather than using a systematic tool. Only 6 out of the 80 studies used a standardized instrument. And in studies that used this instrument, withdrawal effects were found in about half of patients.
References:
- Henssler, J., Schmidt, Y., Schmidt, U., Schwarzer, G., Bschor, T., & Baethge, C. (2024). Incidence of antidepressant discontinuation symptoms: a systematic review and meta‑analysis. The Lancet Psychiatry. Advance online publication. https://doi.org/10.1016/S2215-0366(24)00133-0
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 13 of 24
They also subtracted what they called nocebo withdrawal effects, that is withdrawal effects reported by people coming off placebo, but this is not a like for like situation. Even in their own study, they found that people coming off antidepressants were six times as likely to experience severe withdrawal effects than those people coming off placebo. So it’s not quite clear that it’s reasonable to subtract the less severe withdrawal effects from placebo from the withdrawal effects from antidepressants.
References:
- Henssler, J., Schmidt, Y., Schmidt, U., Schwarzer, G., Bschor, T., & Baethge, C. (2024). Incidence of antidepressant discontinuation symptoms: a systematic review and meta‑analysis. The Lancet Psychiatry. Advance online publication. https://doi.org/10.1016/S2215-0366(24)00133-0
Slide 14 of 24
The other issue with this study is that the average duration of exposure to antidepressants in the studies captured were 25 weeks, so less than six months, whereas we know that patients in the US mostly use these drugs for more than five years. We know that the longer you’re on an antidepressant, the more common and severe withdrawal effects are as for a lot of drugs.
References:
- Henssler, J., Schmidt, Y., Schmidt, U., Schwarzer, G., Bschor, T., & Baethge, C. (2024). Incidence of antidepressant discontinuation symptoms: a systematic review and meta‑analysis. The Lancet Psychiatry. Advance online publication. https://doi.org/10.1016/S2215-0366(24)00133-0
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 15 of 24
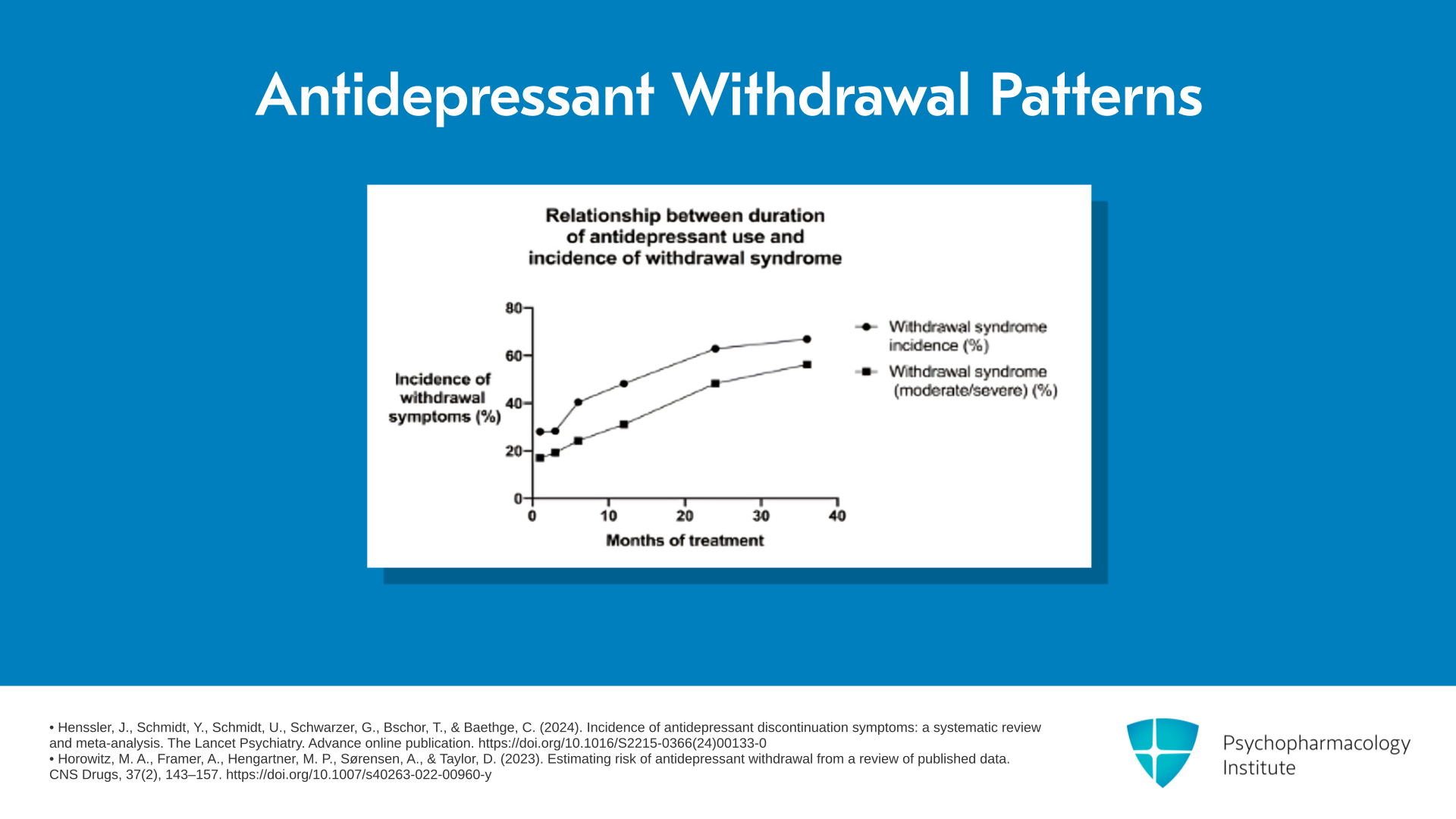
Looking at this graph, this is a simple study in which people were asked: How long were you on an antidepressant before you stopped this? Did you have withdrawal effects? That’s the top line. And were those withdrawal effects moderately severe or severe? That’s that bottom line. And you can see after a few months of use, most people didn’t have withdrawal effects. Only 1 in 3 did. And most people that did have withdrawal effects only had mild symptoms. So only 1 in 5 had moderately severe or severe withdrawal symptoms. Whereas, once people have used the drugs for more than three years, two-thirds of people have withdrawal effects, and half of them are saying that those withdrawal effects are moderately severe or severe. So the Lancet article captured short-term users, whereas the people that we are seeing issues with in clinical practice are this large group of long-term users, now more than 20 million people in the US.
References:
- Henssler, J., Schmidt, Y., Schmidt, U., Schwarzer, G., Bschor, T., & Baethge, C. (2024). Incidence of antidepressant discontinuation symptoms: a systematic review and meta‑analysis. The Lancet Psychiatry. Advance online publication. https://doi.org/10.1016/S2215-0366(24)00133-0
- Horowitz, M. A., Framer, A., Hengartner, M. P., Sørensen, A., & Taylor, D. (2023). Estimating risk of antidepressant withdrawal from a review of published data. CNS Drugs, 37(2), 143–157. https://doi.org/10.1007/s40263-022-00960-y
Slide 16 of 24
So there is, I think, greater recognition that there are withdrawal effects from antidepressants, but there’s still a lack of recognition about the protracted antidepressant withdrawal syndrome, that is, this long-lasting, months or years, syndrome. This can involve all the symptoms in acute withdrawal, panic attacks, sensitivity to light, trouble with balance, anxiety, trouble concentrating. It can be debilitating. People can lose jobs. Relationships can fall apart. People can be bedbound or housebound.
References:
- Hengartner, M. P., Schulthess, L., Sorensen, A., & Framer, A. (2020). Protracted withdrawal syndrome after stopping antidepressants: a descriptive quantitative analysis of consumer narratives from a large internet forum. Therapeutic Advances in Psychopharmacology, 10, 2045125320980573. https://doi.org/10.1177/2045125320980573
- Cosci, F., Mansueto, G., & Fava, G. A. (2020). Relapse prevention in recurrent major depressive disorder. A comparison of different treatment options based on clinical experience and a critical review of the literature. International Journal of Psychiatry in Clinical Practice, 24(4), 341–348. https://doi.org/10.1080/13651501.2020.1779308
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 17 of 24
To highlight this issue, this is from a study we conducted on more than 1000 people and we asked them: What symptoms did you have in the lead up to being prescribed an antidepressant? And what symptoms did you have when you stopped your antidepressant afterwards? And so, for example, you can see that 3 out of 10 people were suicidal in the lead up to being prescribed an antidepressant, but 6 out of 10 were suicidal on stopping the antidepressant. In other words, 3 out of 10 of this group experienced new-onset suicidality only after stopping an antidepressant. And that’s true for every symptom that we looked at.
References:
- Horowitz, M. A., & Taylor, D. (2022). Distinguishing relapse from antidepressant withdrawal: Clinical practice and antidepressant discontinuation studies. BJPsych Advances, 28(5), 297–311. https://doi.org/10.1192/bja.2021.62
- Horowitz, M. A., Framer, A., Hengartner, M. P., Sørensen, A., & Taylor, D. (2023). Estimating risk of antidepressant withdrawal from a review of published data. CNS Drugs, 37(2), 143–157. https://doi.org/10.1007/s40263-022-00960-y
Slide 18 of 24
It was even more marked for other symptoms. So very few people experience brain zaps before starting their drugs and most experience it after stopping. This is a distinct syndrome.
References:
- Horowitz, M. A., & Taylor, D. (2022). Distinguishing relapse from antidepressant withdrawal: Clinical practice and antidepressant discontinuation studies. BJPsych Advances, 28(5), 297–311. https://doi.org/10.1192/bja.2021.62
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 19 of 24
Now, this is a little bit of a tale of two countries, the UK versus the US. So in the last two decades, although the NICE guidelines, that is the official government guidelines in the UK, have described withdrawal effects from antidepressants as brief and mild as they still do today in the US, there have been updates in the UK over the last five years. So in 2019, the world culture psychiatrists actually went on national TV to tell the public that there can be severe and long-lasting withdrawal effects from antidepressants, and the government guideline committee updated its guidelines to say that withdrawal can last for weeks and several months, and can be severe but there hasn’t been any update to the APA guidelines since 2010, and they still say what was thought to be correct now a decade and a half ago.
References:
- Gelenberg, A. J., Freeman, M. P., Markowitz, J. C., Rosenbaum, J. F., Thase, M. E., Trivedi, M. H., & Van Rhoads, R. S. (2010). American Psychiatric Association practice guidelines for the treatment of patients with major depressive disorder. *American Journal of Psychiatry*, *167*(10 Suppl), 9-118. https://doi.org/10.1176/appi.ajp.2010.1001001
- National Institute for Health and Care Excellence. (2022). Medicines associated with dependence or withdrawal symptoms: Safe prescribing and withdrawal management for adults (NICE Guideline NG222). https://tinyurl.com/mw2hv2jr
Slide 20 of 24
There is a way of evaluating someone’s risk of withdrawal. And very briefly, there are four main issues. One is duration of use. So whether someone is a short-term or long-term user has a very big effect on their risk of withdrawal, very low risk for a few months, and very high risk for more than a few years. Different antidepressants have different risks. So particularly SNRIs and paroxetine, and perhaps mirtazapine, have higher risk than other antidepressants although all antidepressants have some risk of withdrawal, and that includes even fluoxetine.
References:
- Horowitz, M., & Taylor, D. M. (2024). The Maudsley deprescribing guidelines: Antidepressants, benzodiazepines, gabapentinoids and Z-drugs. John Wiley & Sons.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 21 of 24
Dosage has some role, low or high doses. High doses have higher risk. And people’s past experience of withdrawal effects, had severe withdrawal symptoms in the past on stopping, then chances are that will happen again in the future.
References:
- Horowitz, M., & Taylor, D. M. (2024). The Maudsley deprescribing guidelines: Antidepressants, benzodiazepines, gabapentinoids and Z-drugs. John Wiley & Sons.
Slide 22 of 24
And based on the Maudsley Deprescribing Guidelines, allows you to work out a risk score for a particular patient and guides you into a rate of reduction.
References:
- Horowitz, M., & Taylor, D. M. (2024). The Maudsley deprescribing guidelines: Antidepressants, benzodiazepines, gabapentinoids and Z-drugs. John Wiley & Sons.
- Horowitz, M. A., Framer, A., Hengartner, M. P., Gomez, A. F., Gel, M., El-Mallakh, R. S., Sharma, T., Holsboer-Trachsler, E., & de Haan, L. (2023). Estimating risk of antidepressant withdrawal from a review of published data. CNS Drugs, 37(2), 143-157. https://doi.org/10.1007/s40263-022-00960-y
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 23 of 24
The key points for this section are: Antidepressant withdrawal symptoms can be severe and long-lasting, months or years. Withdrawal symptoms last for as long as it takes adaptations formed to the presence of the drug to resolve, and not just the time taken for the drug to leave the system, which we know can be months or years from animal and clinical studies.
Slide 24 of 24
And the longer a patient has used an antidepressant, the more likely they are to experience withdrawal symptoms, the more likely they are for those symptoms to be severe and long-lasting. So if people are using the drugs for a few months, they are likely to not have major problems. If people are using the drugs more than a couple of years, they are much more likely to have severe problems coming off their drugs. And some antidepressants like SNRIs and paroxetine have higher risk but all antidepressants have some risk including fluoxetine.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
