Slides and Transcript
Slide 1 of 11
So I'd like to talk a little bit now about assessment and diagnosis of premenstrual mood syndromes.
Slide 2 of 11
I mentioned in the last section that it's really important to understand whether there is a cyclical pattern to symptoms and that the best way to understand that is through prospective ratings of symptoms. And that's because when women are asked to remember something retrospectively, they often don't remember it correctly or they have a key idea in mind that they then apply back to something even if they think they're remembering it correctly. So prospective rating is the most accurate way to get at these symptoms.

Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 11
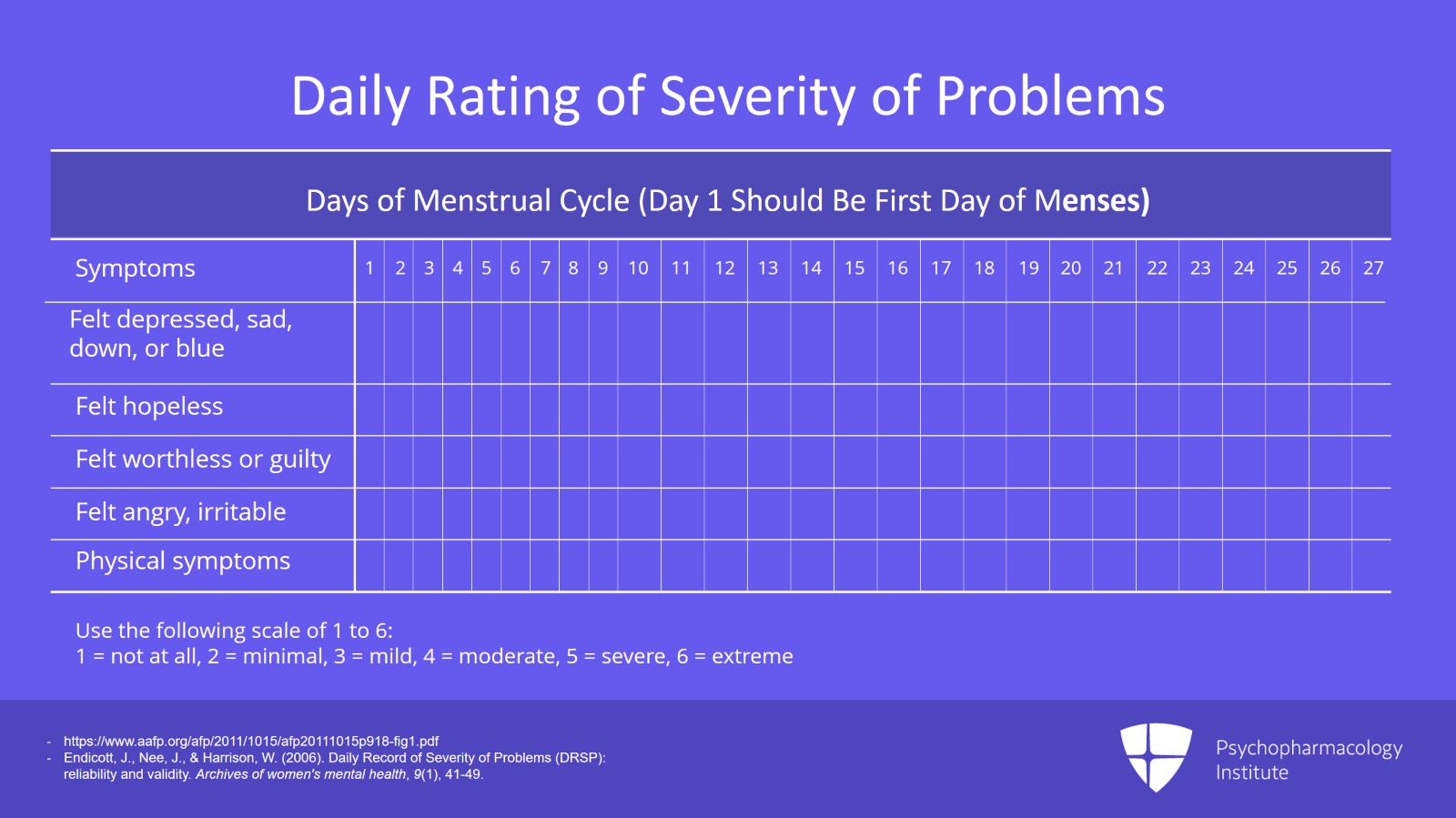
The gold standard for how to prospectively rate these symptoms is an instrument called the Daily Rating of Severity of Problems or the DRSP. This is available online. You can Google it and find it and download it for free. And it's a very systematic rating that shows a whole bunch of different mood symptoms characterized very specifically down the Y axis. And then it has days 1 through 30 horizontally. And the woman is asked to rate each symptom on the different days of the menstrual cycle. So day 1 is the day that she begins to bleed, so the first day of menses. And we ask women to start this on the first day of their next period starting with that day 1. She is supposed to rate with a number 1 to 6, each one of these symptoms. So examples of some of the symptoms are things like felt depressed, sad, down or blue, felt hopeless, felt worthless or guilty, felt angry and irritable. And it includes physical symptoms as well. So if a woman keeps track of this across two or three prospectively charted cycles, we're going to get a real understanding on the scale of 1 to 6 of how well she was doing in terms of these symptoms on each different day of the cycle. And that allows you at a glance to see very quickly whether a woman's symptoms fit into a cyclical pattern or not. It's the most comprehensive tracker available so it's the one that's ideal to use. And if the patient fills it out thoroughly, it's very easy to see whether there's a luteal phase pattern or not and even what type that pattern is. For some women, their symptoms occur beginning two weeks before their period. For some women, it's just three days before their period. And the Daily Record of Severity of Problems will really allow us to see that.
References:
- https://www.aafp.org/afp/2011/1015/afp20111015p918-fig1.pdf
- Endicott, J., Nee, J., & Harrison, W. (2006). Daily Record of Severity of Problems (DRSP): reliability and validity. Archives of women's mental health, 9(1), 41-49.
Slide 4 of 11
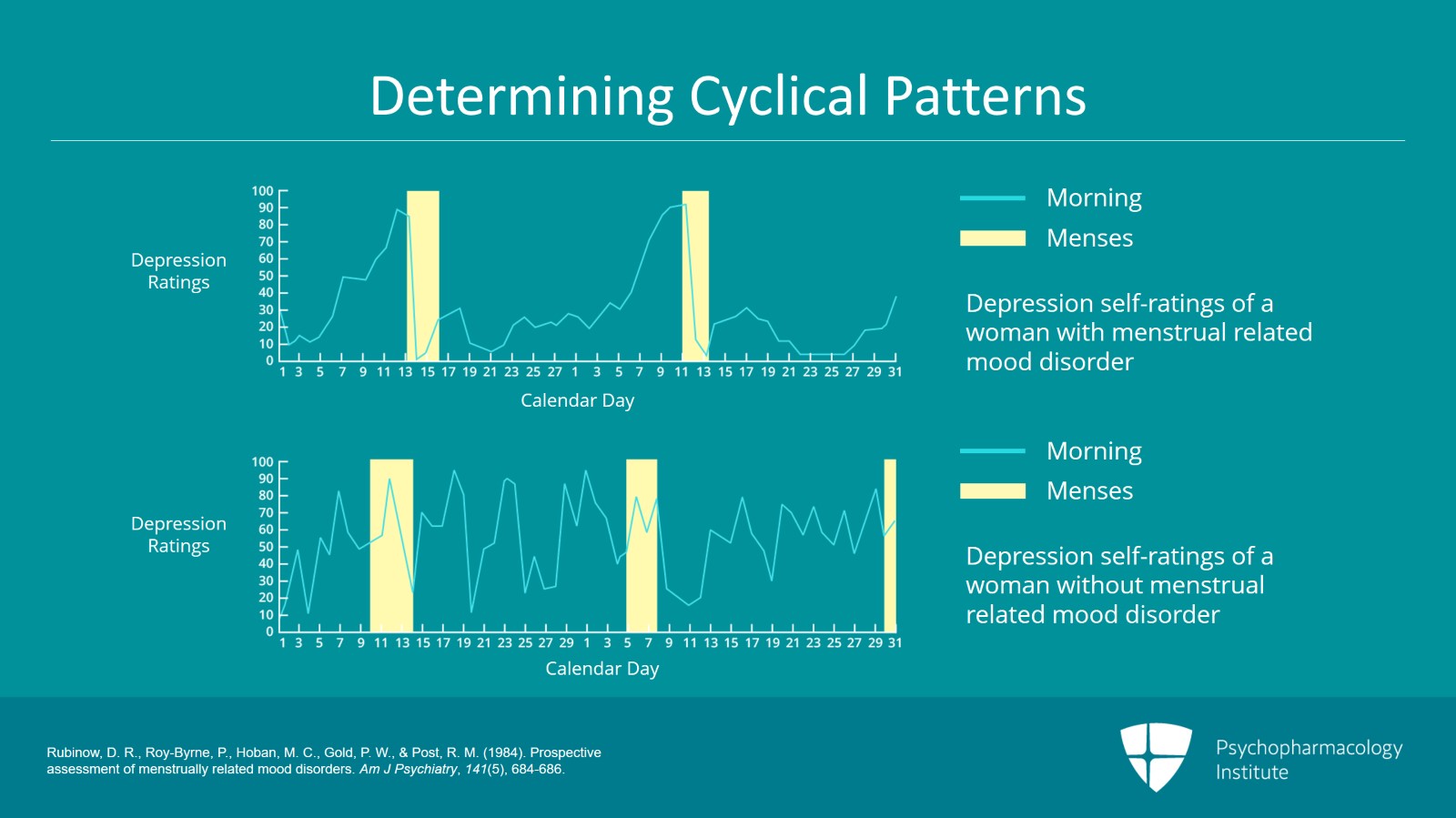
We also need to use these prospective symptom trackers as I said to determine not only the severity of symptoms but whether or not there is a cyclical pattern. And I mentioned that women who have symptoms throughout the month likely have premenstrual exacerbation of another mood disorder rather than PMDD. The exception to that is women who have symptoms that are markedly different in quality and not just severity in the luteal phase. For example, if you have a woman who has let's say an anhedonic melancholic depression most of the time but she becomes very aggressive and irritable in the luteal phase, that might be a woman who has a major depressive disorder and also has PMDD on top of that. So the prospective ratings as you can see are absolutely required to help tease out the differences among these different syndromes. And what I found is that many women who believe they have premenstrual symptoms and do not often do so because of the stigma we have in this country against mental illness. PMS is seen as something more acceptable to have than a psychiatric illness.
References:
- Rubinow, D. R., Roy-Byrne, P., Hoban, M. C., Gold, P. W., & Post, R. M. (1984). Prospective assessment of menstrually related mood disorders. Am J Psychiatry, 141(5), 684-686.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 11
The one problem with it is that patients sometimes find it difficult to adhere to it because you're rating about 30 symptoms on a scale of 1 to 6 across 30 days and it's a lot of work. So one thing that I find useful, a clinical tip, is to ask the patient if she uses an app to track her period. Many young women do. A couple of the apps that I know of out there are Flo and Clue. There are many others. And most of those apps have at least a rudimentary mood tracker. So that can be another way of collecting some prospective information if the patient is unable to complete the more thorough trackers. Many of those trackers will have something like a smiley face or a frowny face. Obviously, that's not as much information as a detailed numbered tracking on 30 different symptoms but at least it's a start. Another useful approach is to design an individualized tracker for that patient depending on her most problematic symptoms. So the clinician can create a simple chart listing the five or six most problematic symptoms and asking the patient to rate them each day of the cycle. In that way, you get something that's individualized to the patient that doesn't ask her to fill out tons of information on something that she may not be experiencing.
References:
- Yonkers, K. A., O'Brien, P. S., & Eriksson, E. (2008). Premenstrual syndrome. The Lancet, 371(9619), 1200-1210.
Slide 6 of 11
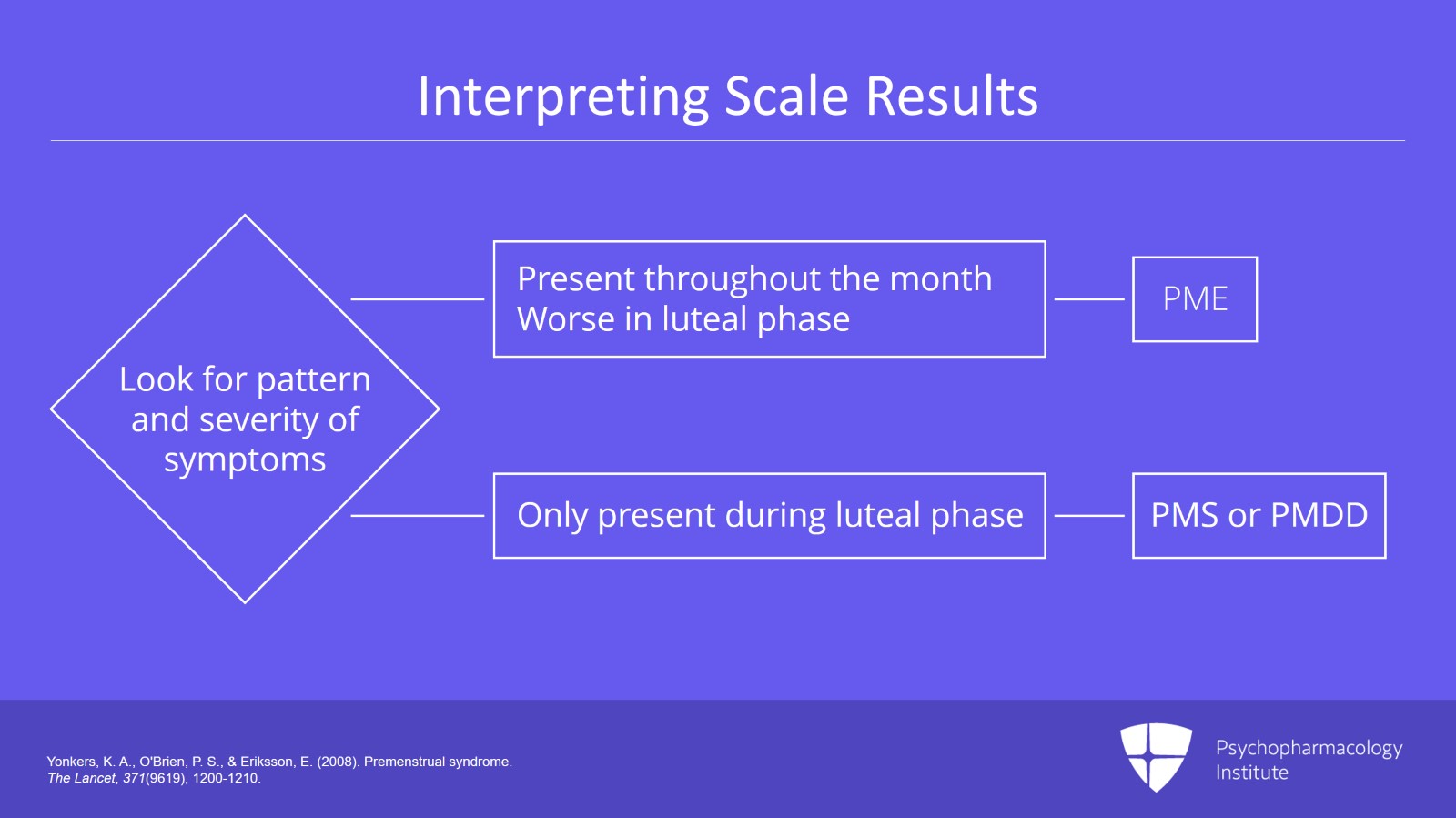
When the clinician is reading the tracker, it's really important to look at both the pattern and the severity. So if there are symptoms throughout the month but they're worse in the luteal phase, that patient likely has premenstrual exacerbation of another mood disorder because she has symptoms throughout the month. If there are symptoms only in the luteal phase and not at any other time, then this is either PMS or PMDD and the severity of symptoms will determine which.
References:
- Yonkers, K. A., O'Brien, P. S., & Eriksson, E. (2008). Premenstrual syndrome. The Lancet, 371(9619), 1200-1210.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 11
There are a number of other assessment tools out there. Some of the ones I'm familiar with are the Calendar of Premenstrual Experience, the Prospective Rating of the Impact and Severity of Menstruation and the Premenstrual Assessment Form and the Penn Daily Symptom Rating. Any of those would be fine to use. As long as you have some kind of symptom tracking, that's better than nothing.
References:
- Mortola, J. F., Girton, L., Beck, L., & Yen, S. S. (1990). Diagnosis of premenstrual syndrome by a simple, prospective, and reliable instrument: the Calendar of Premenstrual Experiences. Obstetrics and Gynecology, 76(2), 302-307.
Slide 8 of 11
Symptom tracking of course isn't the only way that we're going to make this diagnosis. We also want to take a careful psychiatric, gynecologic and medical history. Particularly important will be understanding the family history of other women in her family. Are other women also prone to premenstrual syndromes? We definitely need to test thyroid function to rule out thyroid dysfunction which can contribute to depressive symptoms and can contribute to irregularities in the menstrual cycle as well. There aren't any other laboratory tests needed, however. Hormones that are tested by commercial labs such as estradiol, progesterone, LH and FSH don't actually differ in women with premenstrual symptoms and so they're not useful. Frequently, I will have women come in to my office asking if we can test their hormones because they feel there must be a difference but there isn't actually a difference in those levels. So it's not worthwhile to get those tests.
References:
- Yonkers, K. A., & Simoni, M. K. (2018). Premenstrual disorders. American Journal of Obstetrics and Gynecology, 218(1), 68-74.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 9 of 11
So the key points for this section are understanding that a correct diagnosis is key to determining a treatment plan. We'll talk a little bit later about what's different about treatment among these different syndromes and that getting prospective ratings of symptoms is crucial as many women who report luteal phase symptoms retrospectively do not confirm those symptoms with prospective rating. The Daily Record of Severity of Problems is the most comprehensive data available but it can be difficult for adherence because it requires the patient to do quite a lot. So if the patient can't fill out the DRSP, really any method of tracking symptoms in the luteal phase is fine. Tracking can be tailored to the individual or can be done using a period tracking app which is something that most young women already have.
Slide 10 of 11
If the patient has consistent elevation of symptoms in the luteal phase only with no symptoms at other times, it's PMS or PMDD as opposed to PME. And severity will determine which one of those two syndromes it is.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 11 of 11