Slides and Transcript
Slide 1 of 7
All right. Now, let’s move on to SSRIs. And in particular, are you treating your OCD patients adequately with the SSRIs? So what are the medications of choice for OCD? That’s easy. The top three medications for OCD should be SSRIs, SSRIs or if those fail, you can consider trying SSRIs. This is my little joke but I think it’s important to note that other medications tend not to work as primary treatment for OCD.
Slide 2 of 7
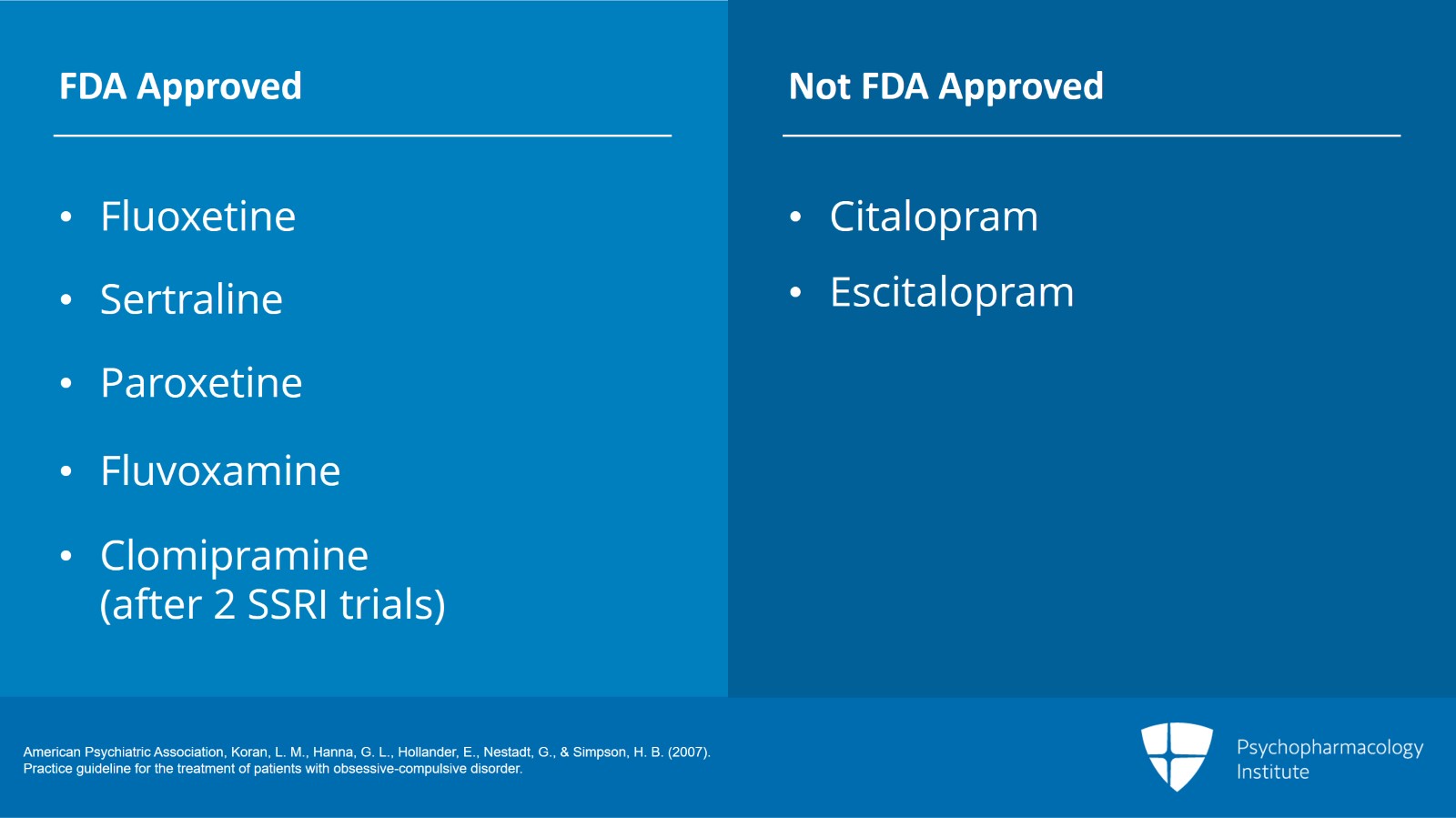
What really works are the serotonin selective reuptake inhibitors as well as a tricyclic medication, clomipramine, that essentially acts like an SSRI as well.
And these are the medications that work for OCD. Other medications outside of the SSRI class have been tried in OCD with relatively mixed success at best. Many medications don’t work at all for OCD. I recommend sticking solely in the SSRI class.
There are five medications approved by the FDA for OCD. That would be fluoxetine, sertraline, paroxetine, fluvoxamine and a medication, clomipramine again which is a TCA that acts like an SSRI. There are two SSRIs that are not FDA approved for adults with OCD but they do work as well, citalopram and escitalopram. Which of these medications do you pick? It does not matter. Again, I recommended above that you try at least two SSRIs before switching to clomipramine.
We consider that to be the third line of a primary medication. Other than that, all of the medications seem to have equal efficacy. All of the SSRIs, there doesn’t seem to be any advantage of one over the other. It really is a matter of side effect profile, other meds that the patient is on and of course clinician preference and patient preference. As I had said before, there may be some advantage to clomipramine over the other SSRIs. It’s a numerical advantage but not necessarily a statistical advantage. We generally hold that out as a third-line medication.
References:
- American Psychiatric Association, Koran, L. M., Hanna, G. L., Hollander, E., Nestadt, G., & Simpson, H. B. (2007). Practice guideline for the treatment of patients with obsessive-compulsive disorder.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 7
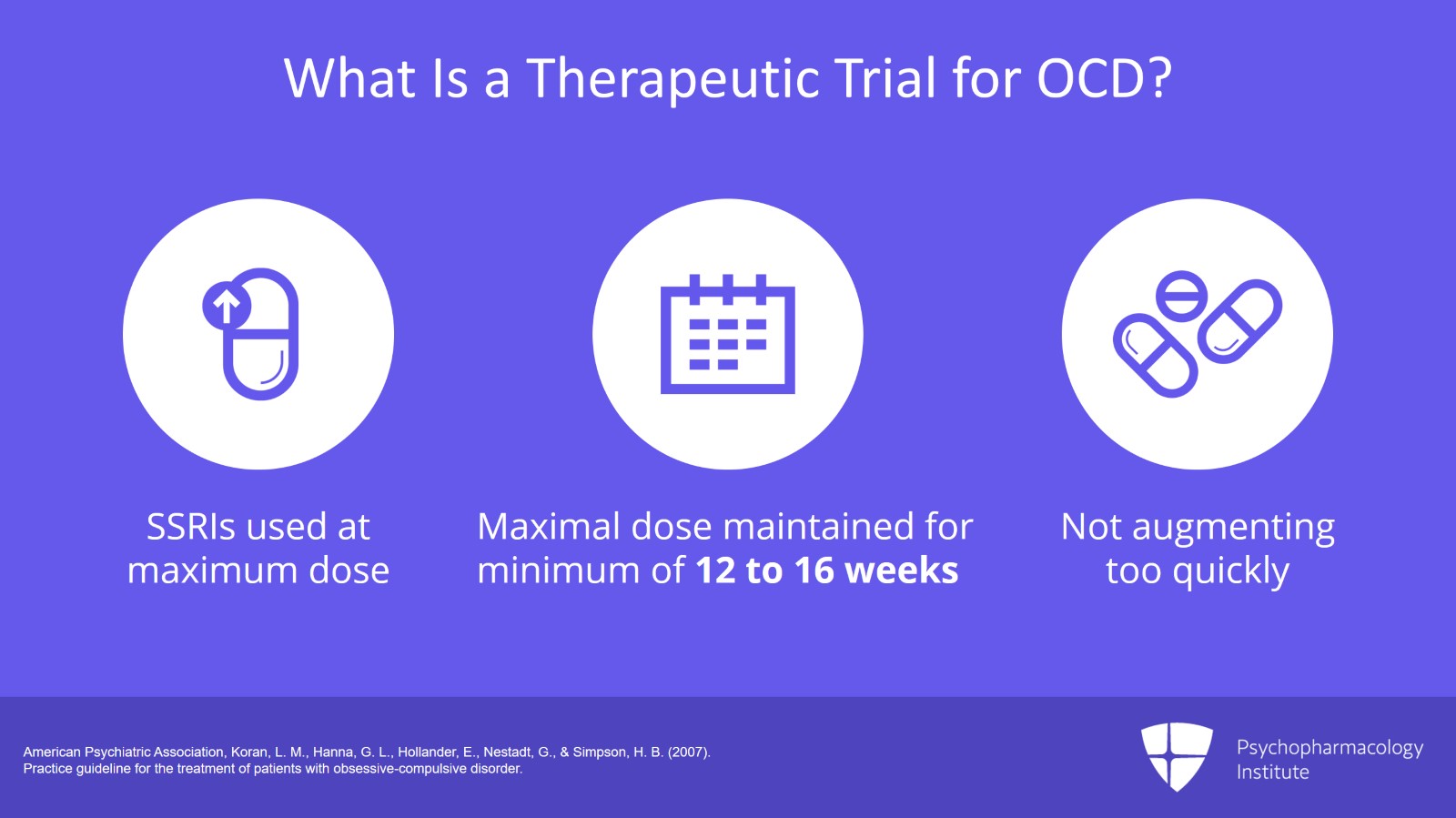
What is a therapeutic trial for OCD? When we’re using SSRIs as primary therapy for OCD, we use them very differently than we use them as antidepressants. Don’t think of SSRIs as antidepressants when you’re treating an OCD patient because the way the medication is used is very different. Patients should be given a therapeutic trial of an SSRI before they’re deemed treatment resistant. I will say in my experience the vast majority of patients that are referred to me and I would say 95% or greater have been given SSRIs but they have been given SSRIs under antidepressant protocols, not anti-obsessional protocols and therefore has not had therapeutic trials.
Therapeutic trial for OCD is very different than what is used as an antidepressant. The SSRIs must be used at a maximal dose and the maximal dose must be maintained for a minimum of 12 to 16 weeks. So often with MDD, we use SSRIs at lower doses but with OCD, it’s very rare that we’re using lower doses. We’re generally pushing the dose up to the maximum dose in the majority of patients. There are some exceptions to that. Sometimes, there are patients who we see who are obviously very treatment responsive at the lower doses. They are certainly the minority of patients and not the majority of patients.
We have all been taught that when using an SSRI as an antidepressant you want to see some response within three to five weeks. That is not the case with OCD. Often, patients with OCD will not even start to respond to the medication until they’ve been on it for at least 12 to 16 weeks only at the maximal dose. Typically, I do not recommend medication augmentation during this time. Even someone who’s gone 10 weeks, 11 weeks, 12 weeks on the highest dose of an SSRI and hasn’t had any response still may respond and still may respond quite well if given enough time. And you can avoid polypharmacy by not being too quick to augment.
References:
- American Psychiatric Association, Koran, L. M., Hanna, G. L., Hollander, E., Nestadt, G., & Simpson, H. B. (2007). Practice guideline for the treatment of patients with obsessive-compulsive disorder.
Slide 4 of 7
So when I’m talking about maximal doses of medications, what am I talking about here?
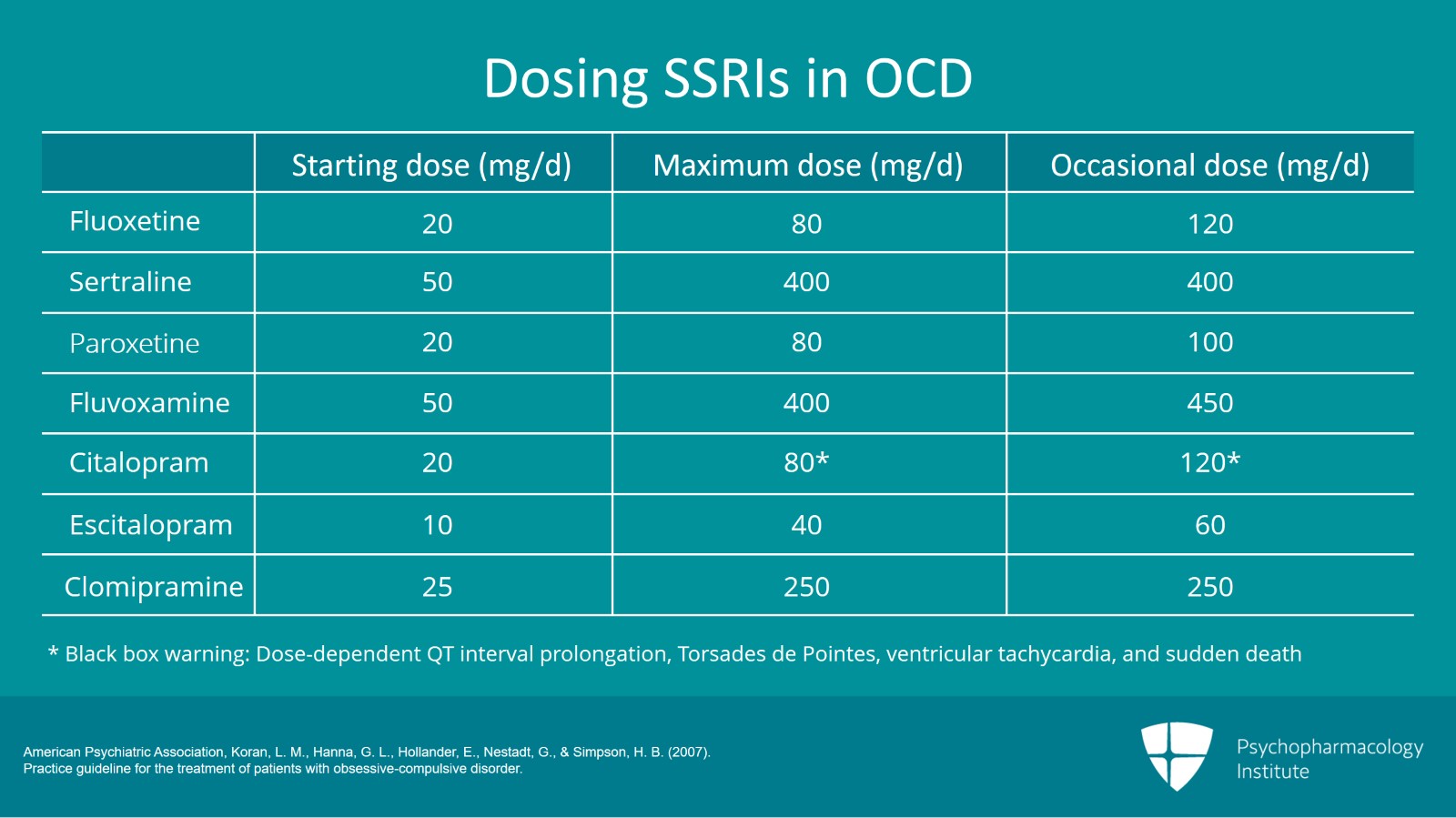
Well, this chart I think lays out some of the medication dosages that I use. So for fluoxetine, while we typically start at 20 mg, most OCD patients should be taken to the maximum dose of 80 mg. There are times for our OCD patients particularly when they have a partial response and would like a greater response, we will take them up to 120 mg. Sertraline is one I want to point out. The maximum dose is 400 mg of sertraline. And all my OCD patients who I start on sertraline, we take them up to 400 mg. That is twice the FDA dose of that medication that is recommended. However, again, the FDA dosing was all done for MDD. And we know that with OCD while some patients do respond at lower doses of 200 mg, many patients require more than that. And 400 mg is a typical maximum dose for sertraline. Many of the other SSRIs I have listed below, their maximum doses are again well above what the FDA recommends but yet these are what is needed for patients with OCD. If you are not using the maximum doses, you’re inadequately treating your patients.
So paroxetine, we go up to 80 mg and often will go as high as 100. With fluvoxamine, we go to 400 and occasionally as high as 450. With citalopram, the maximum dose is 80, occasionally up to 120. I have the asterisk there because of course with recent FDA black box warnings, we don’t usually go that high with citalopram anymore which is why I rarely use citalopram when treating OCD. Escitalopram, while the starting dose is 10, my OCD patients go up to 40 mg as a maximum dose. And it’s not unusual at all for me to have my OCD patients on 60 mg of escitalopram when they have a partial response and really are desiring more response. That is very typical. With clomipramine, the max dose is 250 mg and some clinicians go as high as 300 mg. You do get an increased seizure risk. I generally recommend that most people stick with clomipramine at the 250 mg dose.
These doses as I said are higher than many clinicians are used to. Again, they’re above FDA guidelines which makes clinicians nervous. However, I think it’s important to know that the APA Guidelines specifically state these doses and the APA specifically has these doses as appropriate for OCD usage. There is clinical and research evidence to back these doses up. The FDA doesn’t say that you cannot use these medications at these maximum doses, only that the FDA never approved it. But there is as I said specific guidance from the APA and other organizations that says it’s okay.
References:
- American Psychiatric Association, Koran, L. M., Hanna, G. L., Hollander, E., Nestadt, G., & Simpson, H. B. (2007). Practice guideline for the treatment of patients with obsessive-compulsive disorder.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 7
Key points. SSRIs as well as the TCA clomipramine which acts like an SSRI are the medications of choice for OCD.
Other medications and antidepressants are either less effective or not effective.
The efficacy for all the anti-obsessionals is equivalent except for the possibility that clomipramine may be somewhat superior to the others. The choice of SSRIs is based on side effect profile and preference.
Slide 6 of 7
Doses are typically used at or above the dosing guidelines such as the FDA approved amounts for many of these medications. And patients can be on the medications for three or four months before they even start to notice a response.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 7