
Slides and Transcript
Slide 1 of 10
Let’s talk about educational approaches for patients about sleep and disorders of sleep.
Slide 2 of 10
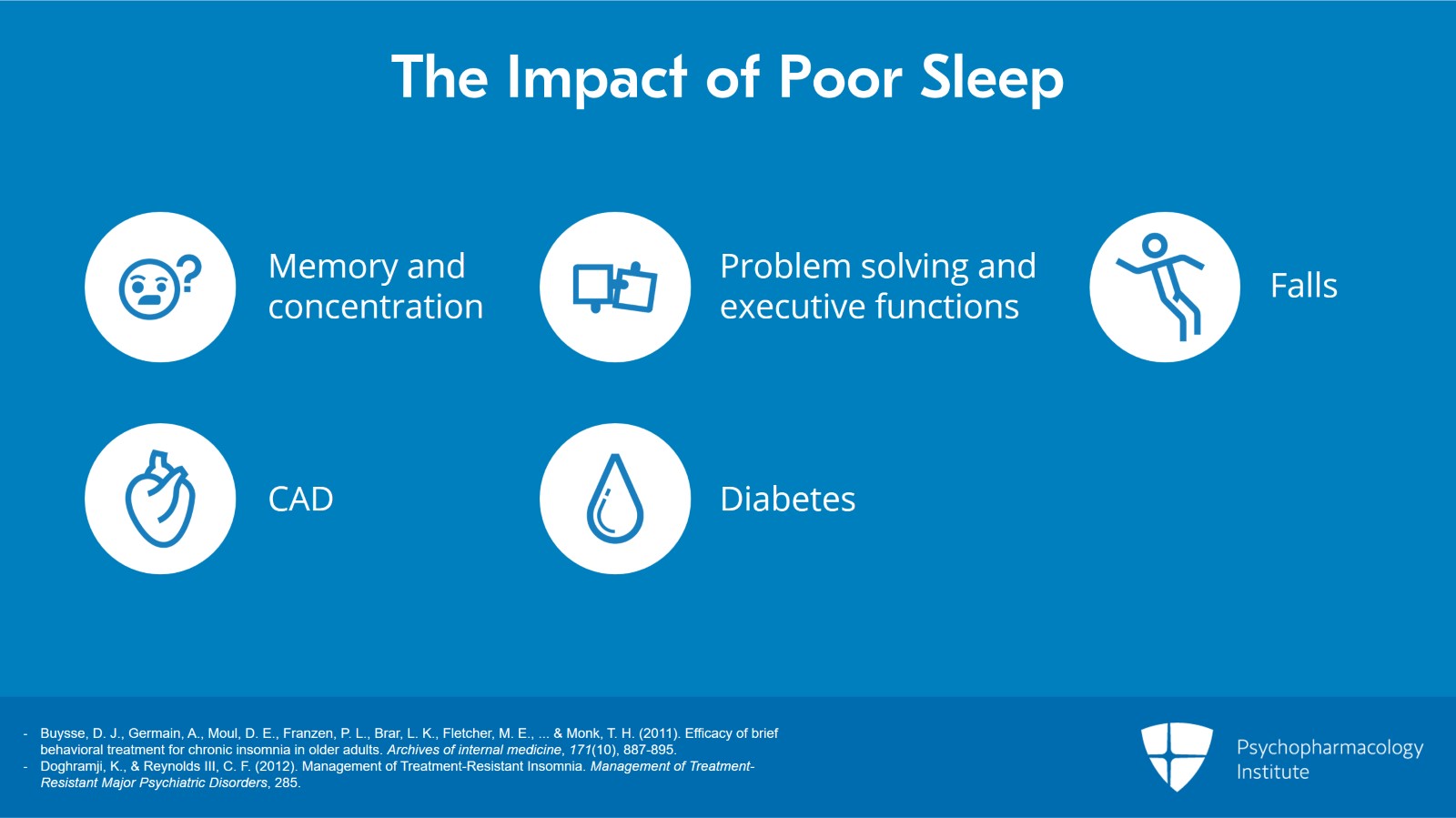
I like to talk to patients and family caregivers concerning the impact of poor sleep. In some cases, these relate to an impact on memory and concentration and on problem solving ability particularly executive functions. There is also, however, an increased risk for falls particularly in older adults who are sleeping poorly. There may be as well an increased risk for coronary artery disease and an increased risk for diabetes mellitus as a result of chronic sleep deprivation. I think the key message here is that sleep quality is critical both to brain health as well as to systemic medical health.
References:
- Buysse, D. J., Germain, A., Moul, D. E., Franzen, P. L., Brar, L. K., Fletcher, M. E., … & Monk, T. H. (2011). Efficacy of brief behavioral treatment for chronic insomnia in older adults. Archives of internal medicine, 171(10), 887-895.
- Doghramji, K., & Reynolds III, C. F. (2012). Management of Treatment-Resistant Insomnia. Management of Treatment-Resistant Major Psychiatric Disorders, 285.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 10
Let’s talk now about the treatment of sleep-wake disorders particularly of insomnia and using a very pragmatic approach called brief behavioral treatment for insomnia.
Brief behavioral treatment for insomnia involves educating the patient about what are healthy sleep practices that is to say lifestyle choices that may promote and protect sleep versus lifestyle choices that tend to interfere with or even to destroy sleep.
Brief behavioral treatment for insomnia or BBTI also is driven by physiological factors that control the depth and continuity of sleep as well as the timing of sleep.
What’s particularly nice about the behavioral interventions that are part of BBTI is that they are deeply anchored in an understanding of the physiological factors that drive sleep and the clocks in the brain that control the timing of sleep and wake. This is a key theme and we’ll come back to it in several ways.
I’d like to credit my colleague at the University of Pittsburgh, Professor Dan Buysse, who developed brief behavioral treatment for insomnia and conducted an important randomized clinical trial that was published in the Archives of Internal Medicine several years ago showing its efficacy in middle aged and older adults seen in primary care practice.
References:
- Buysse, D. J., Germain, A., Moul, D. E., Franzen, P. L., Brar, L. K., Fletcher, M. E., … & Monk, T. H. (2011). Efficacy of brief behavioral treatment for chronic insomnia in older adults. Archives of internal medicine, 171(10), 887-895.
- Doghramji, K., & Reynolds III, C. F. (2012). Management of Treatment-Resistant Insomnia. Management of Treatment-Resistant Major Psychiatric Disorders, 285.
Slide 4 of 10
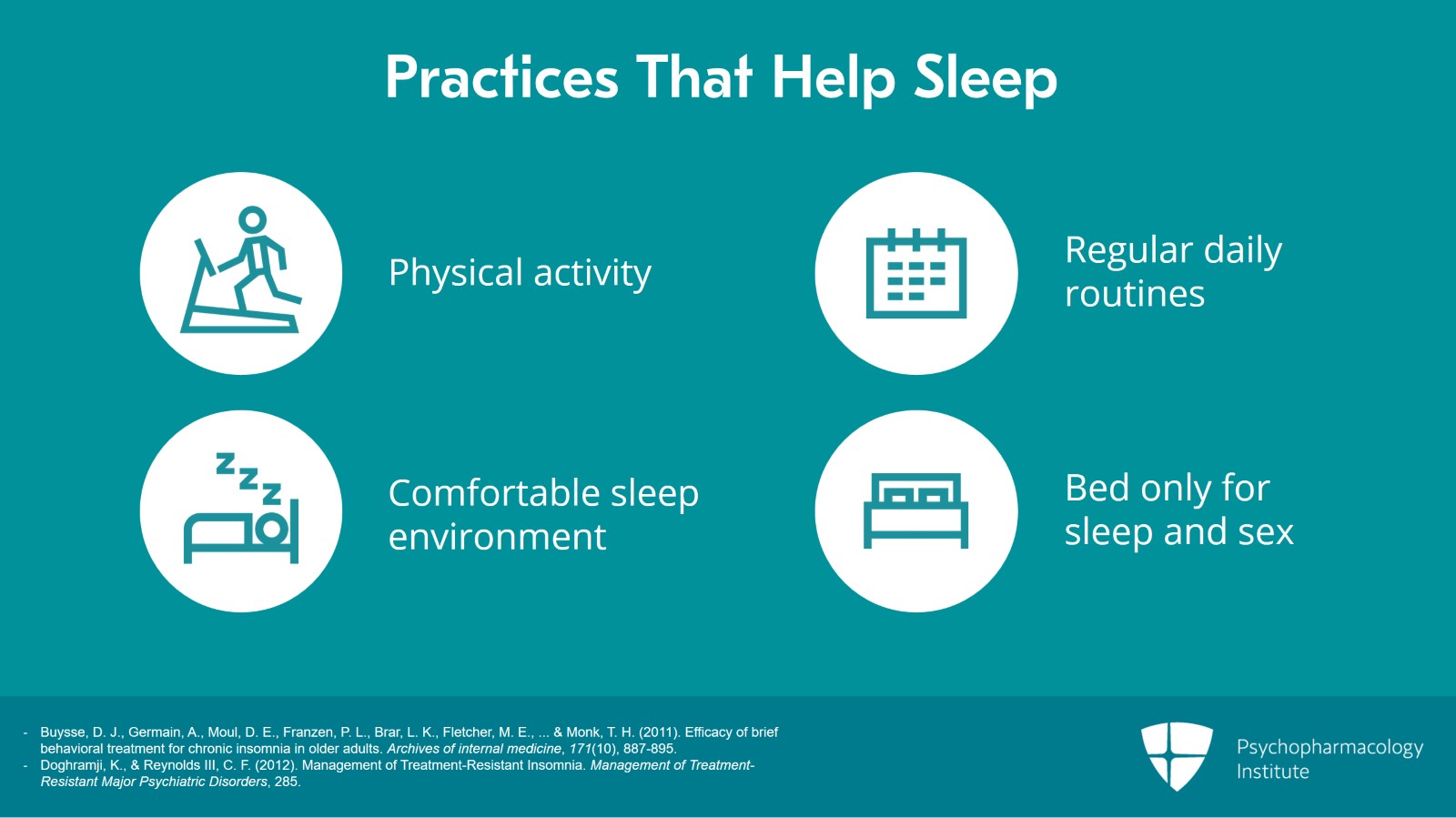
First, with respect to practices that help sleep and again education of patients and their family caregivers is an important part of BBTI, we know that practices that help sleep include physical activity,
It’s probably best to exercise in the morning or in the afternoon hours because exercising in the evening may create alertness or arousal and make it difficult to fall asleep.
Daily routines help keep the brain’s biological clock on time. Having a regular schedule for meals, exercise and other activities is often very helpful.
A comfortable sleep environment is also very important. The room should not be too hot or too cold. People sleep better obviously in dark rooms. People who have trouble sleeping often find that it helps to turn their clock around so that they don’t spend the night watching it.
And finally, people need to remember that the bed is for sleeping and for sex. It’s not for other purposes. If the patient is eating in bed or talking on the phone or watching TV or balancing their checkbook, these are activities that can lead to arousal and make it difficult for the central nervous system to de-arouse to let sleep occur naturally.
References:
- Buysse, D. J., Germain, A., Moul, D. E., Franzen, P. L., Brar, L. K., Fletcher, M. E., … & Monk, T. H. (2011). Efficacy of brief behavioral treatment for chronic insomnia in older adults. Archives of internal medicine, 171(10), 887-895.
- Doghramji, K., & Reynolds III, C. F. (2012). Management of Treatment-Resistant Insomnia. Management of Treatment-Resistant Major Psychiatric Disorders, 285.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 10
Basically, BBTI encourages patients to undertake small changes in their daily lives which decrease arousal and allow the brain’s ability to sleep to emerge. It’s about replacing that vicious cycle that we talked about a few minutes ago with a virtuous cycle that allows normal sleep to occur. Even small changes can help patients sleep better at night and feel better during the day creating a virtuous cycle.
It’s helpful to engage the patient’s bed partner as well in discussions like this and share decision making to encourage persistence in treatment and treatment adherence.
References:
- Buysse, D. J., Germain, A., Moul, D. E., Franzen, P. L., Brar, L. K., Fletcher, M. E., … & Monk, T. H. (2011). Efficacy of brief behavioral treatment for chronic insomnia in older adults. Archives of internal medicine, 171(10), 887-895.
- Doghramji, K., & Reynolds III, C. F. (2012). Management of Treatment-Resistant Insomnia. Management of Treatment-Resistant Major Psychiatric Disorders, 285.
Slide 6 of 10
In contrast to the practices that help sleep, there are practices that hurt sleep and patients need to pay attention to these.
These include the inappropriate use of alcohol, caffeine, worrying, a poor sleep environment and using the bed for things other than sleep or sex.
Alcohol, for example, actually helps people fall asleep more quickly but the problem is that when the alcohol wears off in the middle of the night it actually causes more wakefulness as if you didn’t have any. Alcohol can also lead to the need for urination in the middle of the night. And if you are prone to have sleep apnea, alcohol as a central nervous system depressant can bring out sleep apnea or make it worse.
Patients also need to pay attention to the amount of caffeine that they are consuming. Caffeine can have long-lasting effect for 10 hours or more. It’s also found in many different types of foods and beverages.
References:
- Buysse, D. J., Germain, A., Moul, D. E., Franzen, P. L., Brar, L. K., Fletcher, M. E., … & Monk, T. H. (2011). Efficacy of brief behavioral treatment for chronic insomnia in older adults. Archives of internal medicine, 171(10), 887-895.
- Doghramji, K., & Reynolds III, C. F. (2012). Management of Treatment-Resistant Insomnia. Management of Treatment-Resistant Major Psychiatric Disorders, 285.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 10
Worries are a common cause for insomnia. If your brain is busy thinking or solving problems, it’s difficult to shut it off and to go to sleep. So some people find that it’s helpful to sit down with a pen and paper in the evening, write down the things that worry them and then also jot down a couple of notes about what they can do about these worries the next day and then to allow themselves to relax and to go to sleep. These I think are helpful tips for managing worries at bedtime in order to allow de-arousal to occur.
References:
- Buysse, D. J., Germain, A., Moul, D. E., Franzen, P. L., Brar, L. K., Fletcher, M. E., … & Monk, T. H. (2011). Efficacy of brief behavioral treatment for chronic insomnia in older adults. Archives of internal medicine, 171(10), 887-895.
- Doghramji, K., & Reynolds III, C. F. (2012). Management of Treatment-Resistant Insomnia. Management of Treatment-Resistant Major Psychiatric Disorders, 285.
Slide 8 of 10
Now that we’ve talked a bit about the behaviors that promote or destroy sleep, let’s talk a little bit about the physiological factors that control sleep and there are two of these.
First, how long you’ve been awake and secondly, the brain’s biological clock particularly the clock that resides in the suprachiasmatic nucleus of the hypothalamus.
As you can see, there are two factors that guide our sleep and they usually work together. At the end of the day, our drive to sleep or sleep juice as I like to think of it is high because of how long we’ve been awake and this drives our ability to fall asleep. Then later in the night, our biological clock’s sleep drive helps to reach a peak and helps to stay asleep longer. So these are the basic factors in which brief behavioral treatment for insomnia is based, how long you’ve been awake and the biological clocks that control sleep.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 9 of 10
The key points from a pragmatic perspective are these. By limiting time in bed each night to say six or seven hours and by not taking naps during the day, the brain’s natural drive to sleep is maximized. It allows continuous and deep restorative sleep.
And by maintaining a regular sleep-wake schedule particularly by getting up at the same time each day, an important point of BBTI, the brain’s control of circadian sleep-wake rhythms is anchored and reinforced. This allows a better quality of sleep at night and more alertness and wakefulness during the day.
Slide 10 of 10

Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
