Slides and Transcript
Slide 1 of 13
Section 2, akathisia, how to diagnose it and manage it. So first, I’d like to give a definition of akathisia. It comes from the ancient Greek for not to sit.
Slide 2 of 13
It’s a syndrome that’s often characterized by the inner feeling that one has to move or fidget and people will often shuffle their feet or shift in their chair or get up and pace. The incidence is between 21% and 75% onset after exposure to the drug per year. The prevalence is somewhere between 1 in 5 and maybe as high as 35% or more of patients will develop akathisia when exposed to the medications that cause it.
References:
- Weiden, P. J., Manning, R., Wolfgang, C. D., Ryan, J. M., Mancione, L., Han, G., … & Mayo, M. G. (2016). A randomized trial of iloperidone for prevention of relapse in schizophrenia: the REPRIEVE study. CNS drugs, 30(8), 735-747.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 3 of 13
We know that akathisia is associated with a lower quality of life and as I mentioned earlier discontinuation of treatment. There’s also a literature that suggests that in extreme cases it’s been associated with an increased risk of suicide or even aggressive behavior. And in some geriatric populations, it’s been associated with falls due to the pacing and constant movement.
References:
- Kane, J. M., Fleischhacker, W. W., Hansen, L., Perlis, R., Pikalov III, A., & Assuncao-Talbott, S. (2009). Akathisia: an updated review focusing on second-generation antipsychotics. Journal of Clinical Psychiatry, 70(5), 627.

Slide 4 of 13
The differential diagnosis of akathisia includes anxiety. So anxious patients often wring their hands, fidget or move around as well. Restless legs syndrome is something that should be excluded from the differential diagnoses. Levodopa-induced dyskinesia in patients who might be taking levodopa. Peripheral neuropathy. So if there’s a sensation other than restlessness or the need to move associated like a pain or tingling, be suspicious of peripheral neuropathy.
References:
- Salem, H., Nagpal, C., Pigott, T., & Lucio Teixeira, A. (2017). Revisiting antipsychotic-induced akathisia: current issues and prospective challenges. Current neuropharmacology, 15(5), 789-798.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 5 of 13
Low iron is another condition that can masquerade sometimes as akathisia. Hyperthyroidism. Alcohol or opiate withdrawal is another common one that produces a similar sense of restlessness. And then, stimulant intoxication is something to be evaluated as well.
References:
- Sachdev, P. (1995). The epidemiology of drug-induced akathisia: Part I. Acute akathisia. Schizophrenia bulletin, 21(3), 431-449.
Slide 6 of 13
Now, there are different types of akathisia and these have to do with the timeframe within which they manifest or endure. And so acute akathisia is a duration of six months or less. Chronic is when it persists for six months or more after any dose is changed, up or down. Tardive akathisia is a delayed onset that’s not related to dose change. So for instance, you start the medication at whatever dose and you reach a steady dosing amount. And then within a few months, you see this restlessness emerge. That would be a tardive akathisia. And then withdrawal akathisia is not uncommon. And often, you’ll see this when switching from one antipsychotic to another or after withdrawing anticholinergic medications. So for instance, if you’re using benztropine or trihexyphenidyl to work against drug-induced side effects and let’s say you decrease or withdraw those, sometimes you’ll see akathisia emerge as those medications are reduced.
References:
- Sachdev, P. (1995). The epidemiology of drug-induced akathisia: Part II. Chronic, tardive, and withdrawal akathisias. Schizophrenia bulletin, 21(3), 451-461.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 7 of 13
There’s also this concept that’s been reported in a few case series called pseudoakathisia. And it’s controversial. But essentially, it’s many of the symptoms that go along with akathisia but without the patient’s awareness of that inner restlessness. Again, some people think that it might be just a manifestation of psychomotor agitation or actually tardive dyskinesia and it’s being miscalled akathisia. But essentially, patients are pacing and doing all the things that make them look as if they have akathisia but if you ask them, they don’t have that inner sense of restlessness.
References:
- Sachdev, P. (1995). The epidemiology of drug-induced akathisia: Part II. Chronic, tardive, and withdrawal akathisias. Schizophrenia bulletin, 21(3), 451-461.
Slide 8 of 13
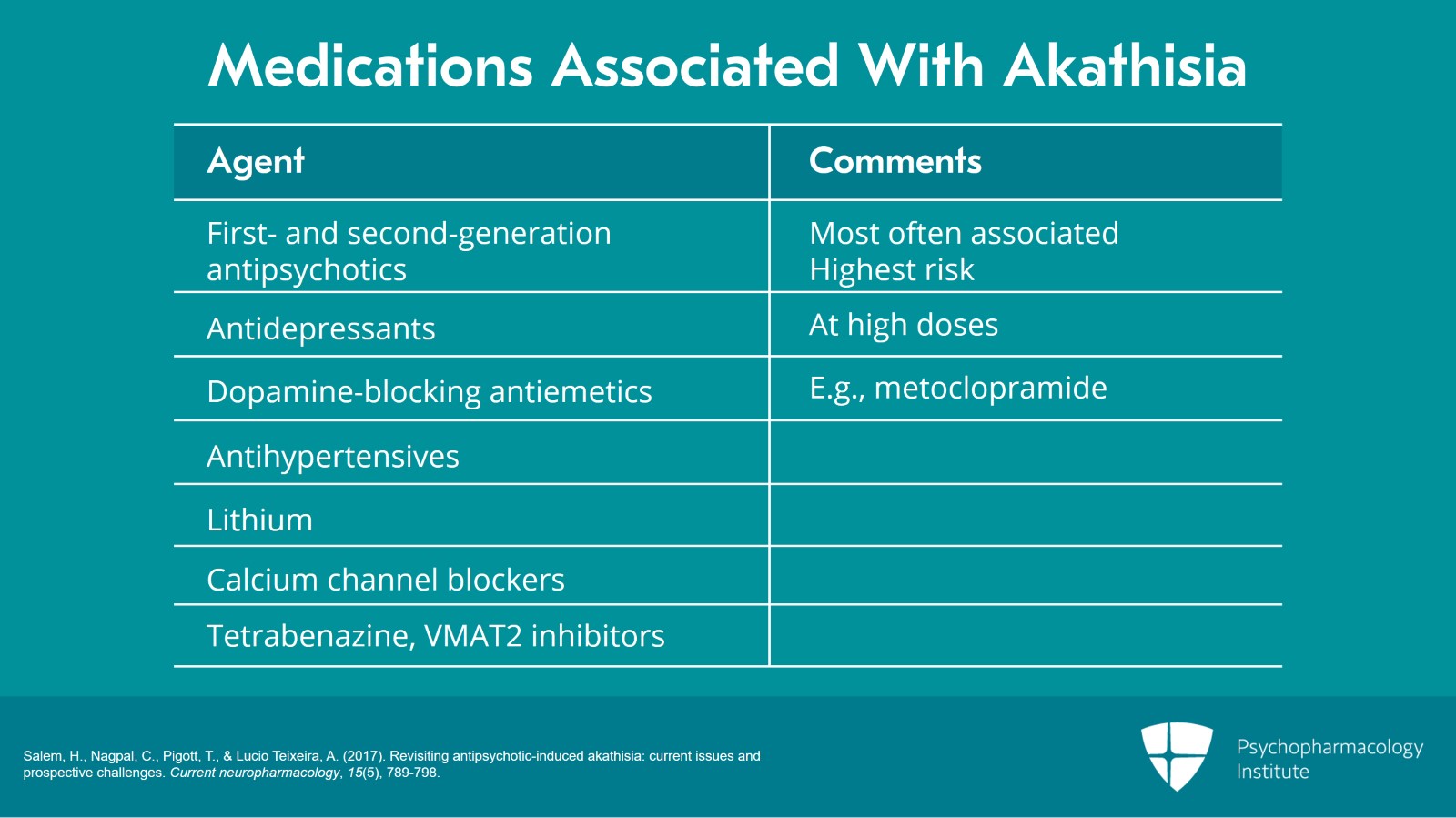
The medications that are most often associated with akathisia are your first- and second-generation antipsychotics. Antidepressants especially at high doses can be associated with akathisia. Dopamine-blocking antiemetics or your metoclopramides are often a cause of the akathisia. Antihypertensives especially things like reserpine or alpha-methyldopa have been associated with akathisia. Lithium. Calcium channel blockers are associated. And tetrabenazine and the VMAT2 inhibitors can cause akathisia. But the highest risk by far and the ones that you’ll see the most reports about are the antipsychotics.
References:
- Salem, H., Nagpal, C., Pigott, T., & Lucio Teixeira, A. (2017). Revisiting antipsychotic-induced akathisia: current issues and prospective challenges. Current neuropharmacology, 15(5), 789-798.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 9 of 13
Now, despite the adverse impact of akathisia, you know, we mentioned that it causes subjective distress in patients and in extreme cases maybe agitation or even increased suicide risk, prophylactic treatment is not generally recommended due to the risk of polypharmacy. And that’s because these other outcomes are less prevalent on average. And so really until you see the symptom of akathisia, it’s better to not start medications prophylactically. So what medications would treat akathisia? We’ll talk about those. But before you introduce a medication, again because we’re really worried about unnecessary polypharmacy, you’re going to want to try to do a few things to mitigate the akathisia before introducing new medications. And so one common thing is to try to lower the medication dose of the causal agent. Another thing that’s commonly tried is to switch antipsychotics. So oftentimes, switching from a first generation or a typical antipsychotic which might have a higher affinity for the D2 receptor to a second-generation antipsychotic might be helpful. The other reason that it also helps is not just the reduced affinity for D2 but also the fact that many of the second-generation antipsychotics have an anticholinergic property that can also work against the akathisia. Again, check for an iron deficiency because remember that’s in the differential diagnoses for akathisia.
References:
- Salem, H., Nagpal, C., Pigott, T., & Lucio Teixeira, A. (2017). Revisiting antipsychotic-induced akathisia: current issues and prospective challenges. Current neuropharmacology, 15(5), 789-798.
Slide 10 of 13
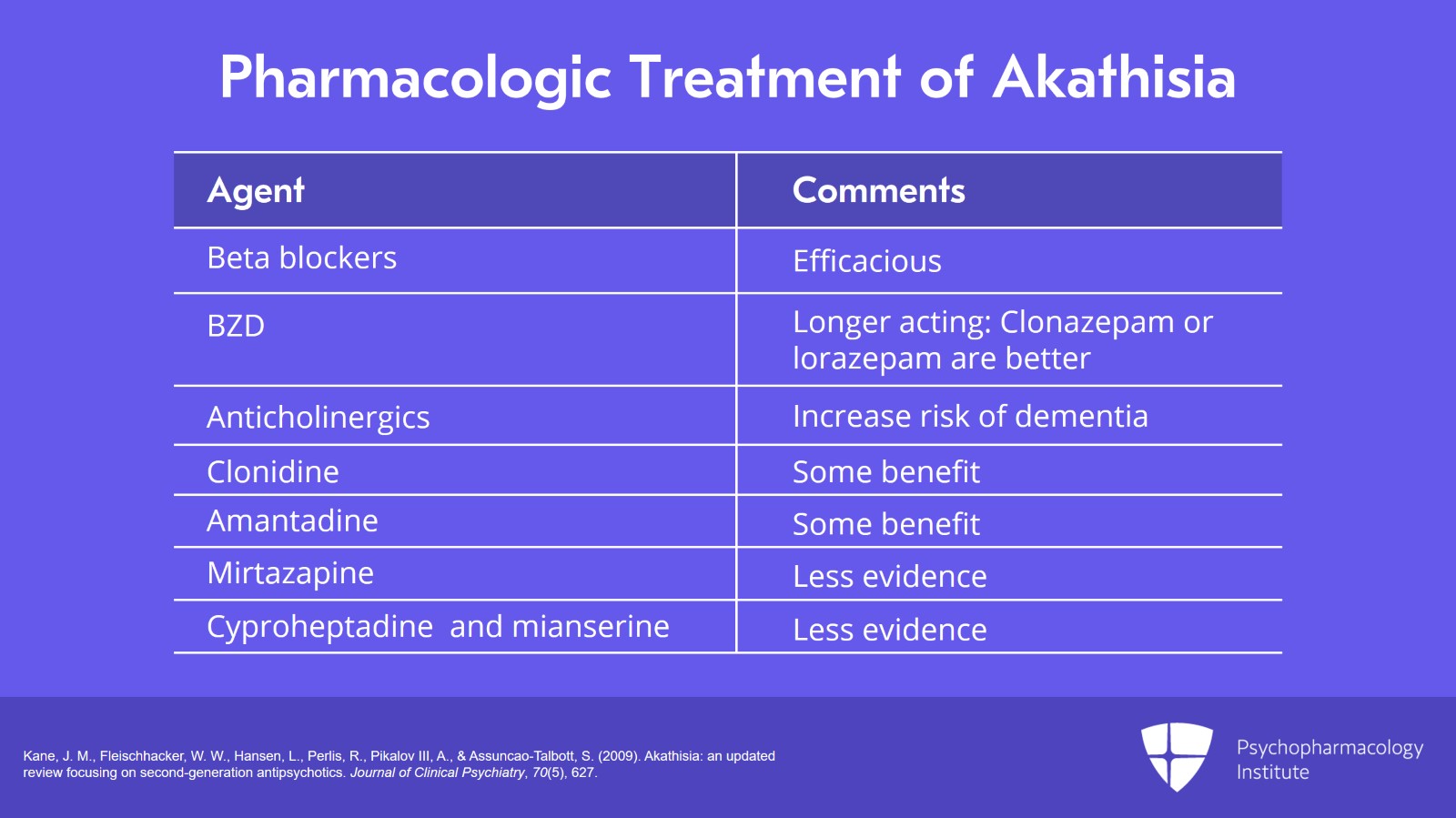
Beta-blockers especially propranolol have shown efficacy in reducing akathisia. Benzodiazepines may be helpful. Typically, we like to go with the longer acting benzodiazepines like clonazepam or lorazepam rather than the shorter acting ones like is alprazolam. Anticholinergic medications, so your benztropine or trihexyphenidyl. However, remember anticholinergics have a range of side effects. They were recently named in a JAMA Internal Medicine article as agents that can increase the risk of dementia later in life. And so use those very judiciously but they certainly can be helpful. Clonidine and amantadine have shown some benefit. And then others that maybe have less evidence from case reports or case series are mirtazapine which is an antidepressant or serotonin antagonists like cyproheptadine and mianserin. So depending on the acuity of the clinical illness that you’re treating, treatment of akathisia should begin with a determination of whether the suspected causal agent can be reduced to eliminate the akathisia. Obviously, if someone is acutely psychotic and agitated, it’s going to be difficult to lower the dose. So you want to be cautious. But in situations where reduction of the causal agent either doesn’t help or isn’t clinically indicated, you want to then at that point go ahead and start looking at some of these options I just mentioned, the beta-blockers, benzodiazepines, anticholinergics, clonidine and amantadine, possibly in that order because that’s aligned pretty much in the order of evidence to treat the akathisia.
References:
- Kane, J. M., Fleischhacker, W. W., Hansen, L., Perlis, R., Pikalov III, A., & Assuncao-Talbott, S. (2009). Akathisia: an updated review focusing on second-generation antipsychotics. Journal of Clinical Psychiatry, 70(5), 627.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 11 of 13
So the key points are that akathisia occurs in about 1/3 of patients treated chronically for mental illness. Akathisia is associated with side effects and treatment discontinuation. So once it’s recognized, you should aggressively manage it.
Slide 12 of 13
And then treating akathisia may include reducing the dose of the causal agent or switching treatment for ones that have a lower liability for causing the akathisia. And then finally, if these things don’t work or not clinically tenable, add a medication to treat akathisia.
Free Files
Download PDF and other files
Success!
Check your inbox, we sent you all the materials there.
Slide 13 of 13