Learning Objectives:
After completing this activity, the learner will be able to:
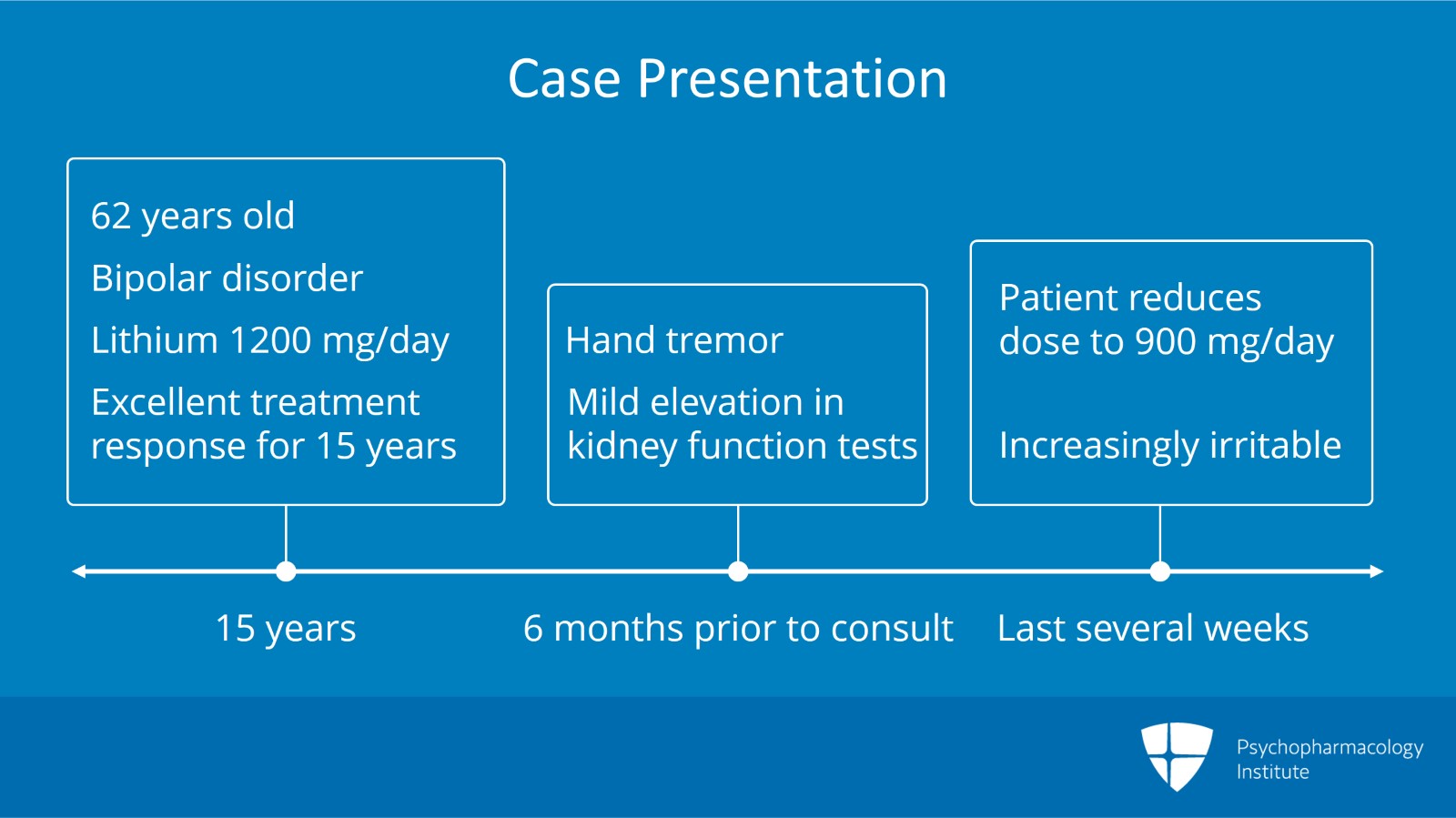
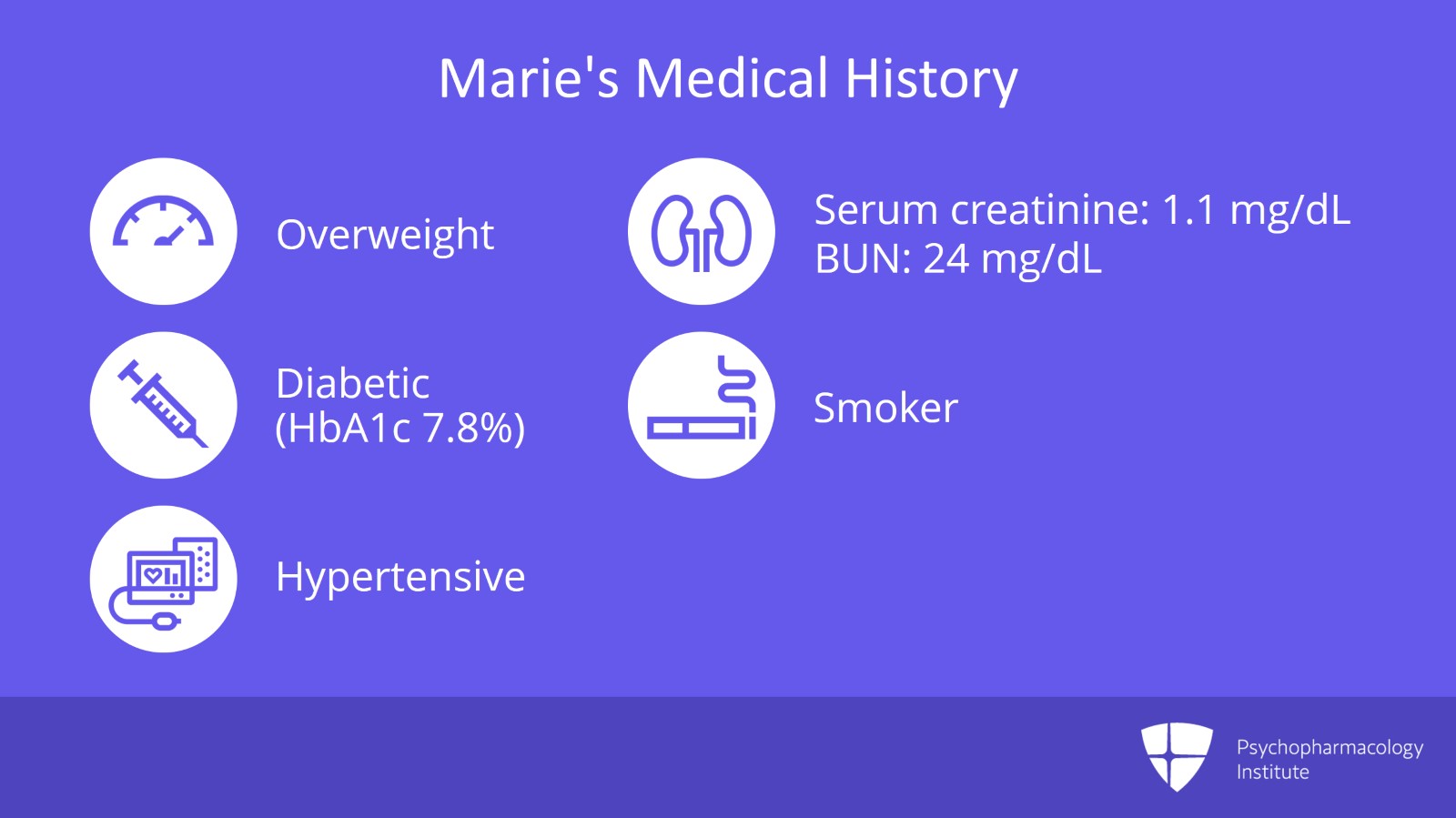
- Identify patients with older-age bipolar disorder (OABD) and be aware of how medical comorbidities can affect outcomes and treatment.
- Recognize that patients with OABD need careful monitoring of treatment due being more prone to side effects and interactions with other medications.
Original Release Date: October 8, 2019
Expiration Date: March 31, 2022
Relevant Financial Disclosures:
Martha Sajatovic declares the following interests:
- Otsuka, Alkermes, Janssen, International Society for Bipolar Disorders, Reuter Foundation, Woodruff Foundation, Reinberger Foundation, National Institutes of Health (NIH), Centers for Disease Control and Prevention (CDC): Contracted research
- Alkermes, Bracket, Otsuka, Janssen, Neurocrine, Health Analytics, Frontline Medical Communications: Consulting activities
- Springer Press, Johns Hopkins University Press, Oxford Press, UpToDate: Publications
- American Physician?s Institute, MCM Education, CMEology, Potomac Center for Medical Education, Global Medical Education, Creative Educational Concepts, Psychopharmacology Institute: Development of CME materials
All of the relevant financial relationships listed above have been mitigated by Medical Academy and the Psychopharmacology Institute.
Contact Information: For questions regarding the content or access to this activity, contact us at support@psychopharmacologyinstitute.com